Health and Access to Care Among Employed and Unemployed Adults: United States, 2009–2010
On This Page
- Key findings
- Unemployed adults aged 18–64 years were less likely to have private insurance and more likely to be uninsured than employed adults.
- Unemployed adults in 2009–2010 were more likely to have fair or poor health than employed adults across all categories of insurance coverage.
- Unemployed adults were more likely to have serious psychological distress than employed working-age adults, regardless of health insurance coverage.
- Unemployed adults had more difficulties obtaining needed medical care due to cost than employed adults, regardless of insurance coverage.
- Unemployment was associated with reduced access to needed prescription drugs due to cost.
- Summary
- Definitions
- Data source and methods
- About the authors
- References
- Suggested citation
 (530 KB)
(530 KB)Anne K. Driscoll, Dr.P.H., and Amy B. Bernstein, Sc.D.
Key findings
Data from the National Health Interview Survey, 2009–2010- In 2009–2010, 48.1% of unemployed adults aged 18–64 years had health insurance compared with 81.4% of employed adults; among the insured, a higher proportion of the unemployed had public insurance.
- Unemployed adults had poorer mental and physical health than employed adults; this pattern is found for insured and uninsured adults.
- Unemployed adults were less likely to receive needed medical care due to cost than the employed in each insurance category.
- The unemployed were less likely to receive needed prescriptions due to cost than the employed in all insurance categories.
- Uninsured adults were less likely to receive needed medical care and prescription drugs due to cost than those with public or private insurance, regardless of employment status.
Keywords: health insurance • employment • health • access to care
full-text:
Products - Data Briefs - Number 83 - January 2012
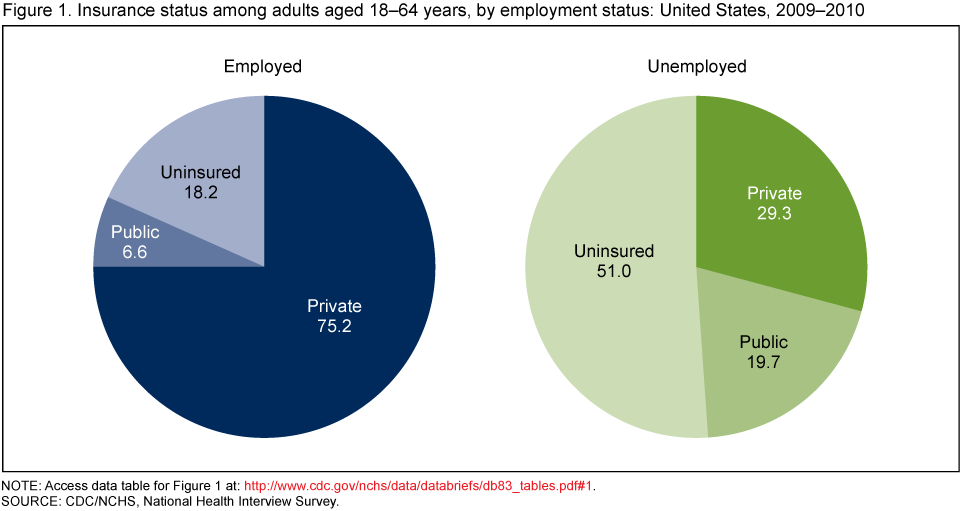
Unemployed adults aged 18–64 years were less likely to have private insurance and more likely to be uninsured than employed adults.
- In 2009–2010, three quarters (75.1%) of employed adults aged 18–64 years had private health insurance coverage; more than four in five (81.4%) had either public or private insurance (Figure 1).
- Less than one-half (48.1%) of unemployed adults had any health insurance coverage. Of those with coverage, 59% had private coverage and 41% had public health insurance.
- Unemployed adults were more likely to be non-Hispanic black, to have less than a high school education, and to have family income below the poverty level in the previous year than employed adults (Appendix table).
NOTE: Access data table for Figure 1
[PDF - 21 KB].SOURCE: CDC/NCHS, National Health Interview Survey.
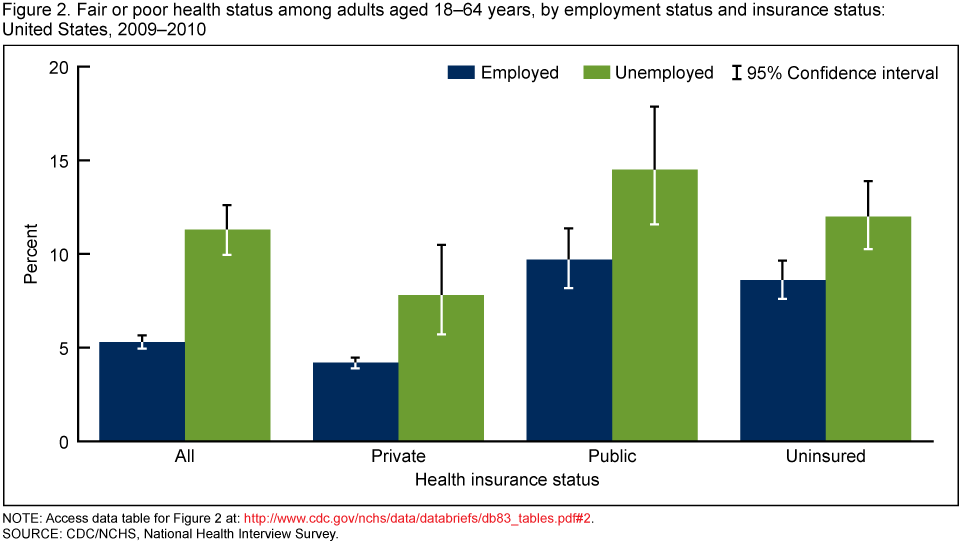
Unemployed adults in 2009–2010 were more likely to have fair or poor health than employed adults across all categories of insurance coverage.
- Overall, 11.3% of unemployed adults aged 18–64 years had fair or poor health compared with 5.3% of employed adults (Figure 2).
- Among adults with private insurance, 4.3% of employed adults had respondent-reported fair or poor health compared with 7.8% of the unemployed. Among those with public insurance, 1 in 10 (10.2%) employed adults had fair or poor health compared with 1 in 7 (14.7%) unemployed adults.
- Adults with public health insurance and the uninsured were more likely to have fair or poor health than those with private coverage, regardless of employment status.
NOTE: Access data table for Figure 2
[PDF - 21 KB].SOURCE: CDC/NCHS, National Health Interview Survey.
Unemployed adults were more likely to have serious psychological distress than employed working-age adults, regardless of health insurance coverage.
- Overall, 6.3% of unemployed adults aged 18–64 years reported serious psychological distress compared with 1.7% of employed adults (Figure 3).
- Among adults with private health insurance, unemployed persons were more than three times as likely to experience serious psychological distress as their employed peers (4.8% versus 1.3%); and among those with public health insurance, the unemployed were almost three times as likely to suffer serious psychological distress as the employed (8.7% compared with 3.1%).
- Adults with public health insurance and the uninsured were more likely to suffer serious psychological distress than those with private insurance, regardless of employment status.

NOTE: Access data table for Figure 3
[PDF - 21 KB].SOURCE: CDC/NCHS, National Health Interview Survey.
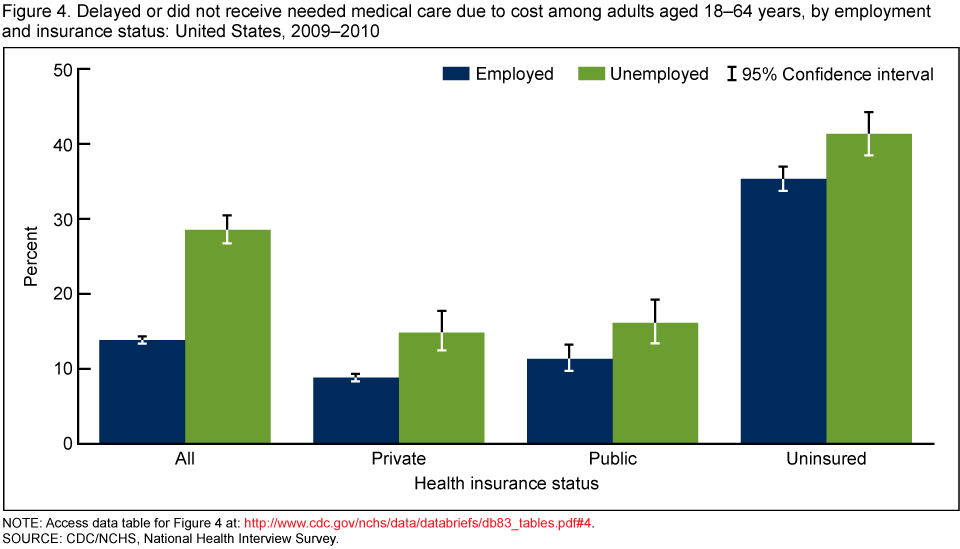
Unemployed adults had more difficulties obtaining needed medical care due to cost than employed adults, regardless of insurance coverage.
- Among adults with private health insurance, one in seven (14.7%) unemployed adults experienced either a delay or lack of needed medical care because of cost compared with 8.7% of employed adults (Figure 4).
- Among adults with public health insurance, one in six (16.0%) unemployed adults reported a cost-related delay or lack of needed medical care compared with one in nine (11.2%) employed adults.
- Uninsured adults were more likely to experience delayed or no needed medical care than adults with either private or public health insurance. This pattern holds among both the employed and unemployed. Among unemployed adults, two-fifths (41.2%) of the uninsured experienced a delay or lack of needed medical care compared with 16.0% of those with public coverage and 14.7% of those with private coverage.
NOTE: Access data table for Figure 4
[PDF - 21 KB].SOURCE: CDC/NCHS, National Health Interview Survey.
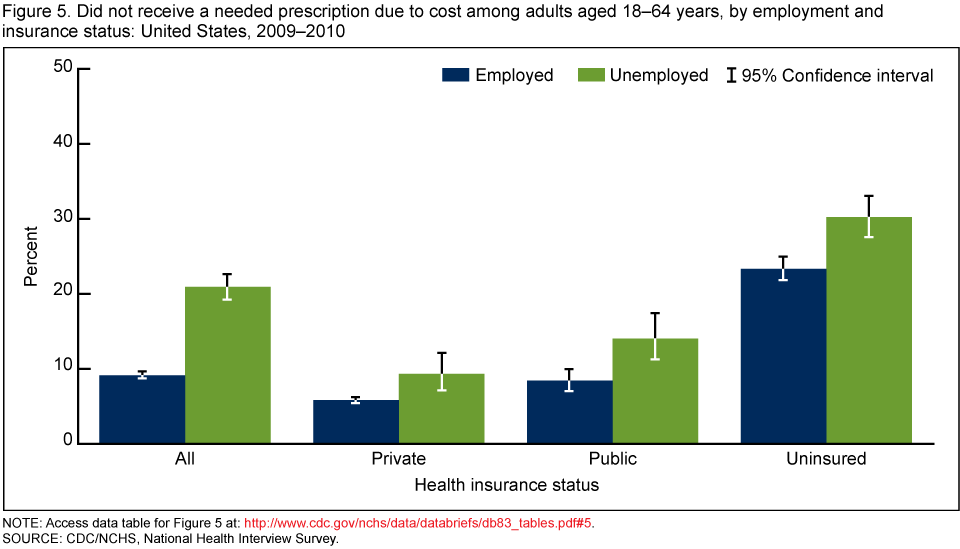
Unemployment was associated with reduced access to needed prescription drugs due to cost.
- Among those with private health insurance, 5.7% of employed adults did not get needed prescriptions because they could not afford them compared with 9.2% of unemployed adults (Figure 5).
- Similarly, among those with public health insurance, 1 in 12 (8.3%) employed adults did not get needed prescriptions compared with almost 1 in 7 (13.9%) of unemployed adults.
- Three in 10 (30.1%) unemployed uninsured adults did not get a needed prescription in the past year compared with 23.2% of employed uninsured adults.
- Adults without health insurance, both employed and unemployed, were more than twice as likely to not get needed prescription drugs because they could not afford them as those with either public or private insurance. Among unemployed adults, 3 in 10 (30.1%) of the uninsured did not get needed prescription drugs due to cost compared with 13.9% of those with public coverage and 9.2% of those with private coverage.
NOTE: Access data table for Figure 5
[PDF - 21 KB].SOURCE: CDC/NCHS, National Health Interview Survey.
Summary
Lack of health insurance has been shown to be associated with problems obtaining needed health care (3), and the unemployed are less likely to have health insurance than are their employed counterparts. The number and rate of adults aged 18–64 years lacking health insurance has been increasing, in part due to the historically high unemployment rates. However, even having comprehensive health insurance coverage does not guarantee access to needed services, in part because of cost-sharing, including copayments and deductibles. Unemployed persons may retain their health insurance through the Consolidated Omnibus Budget Reconciliation Act (COBRA) or through other programs, but COBRA payments in particular may be quite expensive, and individual insurance plans may be less comprehensive than many employer-sponsored plans (4). Thus, although some unemployed adults may retain coverage for some period of time, they may be less able to meet cost-sharing requirements because of reduced income associated with unemployment.This analysis compares the health status and access to care of employed and unemployed adults and shows that unemployment is associated with unfavorable health and access to care among adults in the labor force over and above the loss of health insurance. However, it is not possible to know from these data the extent to which unemployment is a cause or effect of poor health. Poor health may be both a cause and effect of unemployment. Adults with private health insurance were more likely to have serious psychological distress and respondent-reported fair or poor health status if they were unemployed. In fact, unemployed privately insured persons were more than three times as likely to have serious psychological distress as their employed counterparts. Similar patterns were found for adults with public insurance and no health insurance. There were no significant differences between employed and unemployed adults in the percentage who had ever been diagnosed with selected chronic conditions, including hypertension, heart disease, diabetes, or cancer (NCHS unpublished analysis of NHIS data), and so the need for health care to treat these chronic conditions exists for both employed and unemployed adults.
In addition to having poorer health, unemployed adults were more likely to delay or not receive needed medical care and needed prescriptions due to cost than their employed counterparts across categories of insurance coverage. Thus, the unemployed reported both worse health and less access to needed care and treatment than employed adults. This pattern was found not only for those without health insurance but also those with public and private insurance.
Definitions
Unemployed and employed: NHIS respondents were asked "What was [person]/were you doing last week?" for each person aged 18 and older. Those who were "looking for work" were classified as unemployed. Those who were "working for pay at a job or business," "with a job or business but not at work," or "working, but not for pay, at a family-owned job or business" were classified as employed. Persons "not working at a job or business and not looking for work" were not in the labor force and are not included.Insurance: Measured at time of interview. Private insurance is coverage obtained through an employer, union, or individual purchase. Public insurance is Medicaid, Medicare, other government-sponsored programs, or a military health plan (TRICARE, VA, or CHAMP-VA). Adults covered by both private and public insurance were considered to have private insurance. Persons without private or public insurance and those with only Indian Health Service coverage or only a private plan that paid for one type of service such as accidents or dental care are considered uninsured.
Health status: Measured by asking the family respondent about his/her health or the health of a family member: "Would you say [person's] health in general is excellent, very good, good, fair, or poor?"
Serious psychological distress: The K6 instrument measures psychological distress associated with unspecified but potentially diagnosable mental illness. Serious psychological distress during the past 30 days is defined as a score of 13 or more on the K6 instrument (5).
Access to medical care: Measured by asking the family respondent: "During the past 12 months, has medical care been delayed for [person] because of worry about the cost?" and "During the past 12 months, was there any time when [person] needed medical care, but did not get it because [person] couldn't afford it?" If the answer to either question was 'yes', participants experienced a delay or lack of care.
Access to prescription medicines: Measured by asking sample adults: "During the past 12 months, was there any time when you needed any of the following, but didn't get it because you couldn't afford it?" "Prescription medicine" is one possible response.
Data source and methods
Data from the 2009 and 2010 National Health Interview Survey (NHIS) were combined for this analysis. NHIS data are collected continuously throughout the year for the Centers for Disease Control and Prevention's (CDC) National Center for Health Statistics (NCHS), by interviewers from the U.S. Census Bureau. NHIS collects information about the health and health care of the civilian, noninstitutionalized U.S. population. Interviews are conducted in respondents' homes, but follow-ups to complete interviews may be conducted over the telephone. The family component collects information on all family members and the sample adult component collects additional data on a randomly selected adult (the "sample adult"). Most information presented in this data brief was reported by a family respondent in the family component of the survey. Questions on serious psychological distress and access to prescription drugs were self-reported by the sample adult. All estimates in this report are based on data for sample adults. For further information about NHIS and the questionnaire, visit the NHIS website.NHIS is designed to yield a sample representative of the civilian noninstitutionalized population of the United States, and this analysis uses weights to produce national estimates. Point estimates and estimates of corresponding variances for this analysis were calculated using SUDAAN software to account for the complex sample design of the NHIS. All estimates shown in this report have a relative standard error less than or equal to 30%. Differences between percentages were evaluated using two-sided significance tests at the 0.05 level with no adjustment for multiple comparisons. Terms such as "higher than" and "less than" indicate statistically significant differences. Terms such as "similar" and "no difference" indicate that the statistics being compared were not significantly different. Lack of comment regarding the difference between any two statistics does not necessarily suggest that the difference was tested and found to be not significant.
About the authors
Anne K. Driscoll and Amy B. Bernstein are with CDC's NCHS, Division of Analysis and Epidemiology.References
- National Bureau of Economic Research (NBER), Business Cycle Dating Committee. Memo, September 20, 2010
.
- Bureau of Labor Statistics (BLS). Household Data Annual Averages; Table 1. Employment status of the civilian noninstitutional population, 1940 to date
- Fronstin P. The impact of the recession on employment-based health coverage. EBRI Issue Brief, no. 342. Employee Benefit Research Institute, Washington, DC. 2010.
- Holahan J, Garrett AB. Rising unemployment, Medicaid and the uninsured. Washington, DC: Kaiser Commission on Medicaid and the Uninsured, The Urban Institute. 2009.
- Kessler RC, Barker PR, Colpe LJ, Epstein JF, Gfroerer JC, Hiripi E, et al. Screening for serious mental illness in the general population. Arch Gen Psychiatry 60(2):184–9. 2003.
Suggested citation
Driscoll AK, Bernstein AB. Health and access to care among employed and unemployed adults: United States,2009–2010. NCHS data brief, no 83. Hyattsville, MD: National Center for Health Statistics. 2012.
Copyright information
All material appearing in this report is in the public domain and may be reproduced or copied without permission; citation as to source, however, is appreciated.National Center for Health Statistics
Edward J. Sondik, Ph.D., DirectorJennifer H. Madans, Ph.D., Associate Director for Science
Office of Analysis and Epidemiology
Diane M. Makuc, Dr.P.H., Acting Directorfull-text:
Products - Data Briefs - Number 83 - January 2012
No hay comentarios:
Publicar un comentario