State-Level and County-Level Estimates of Health Care Costs Associated with Food Insecurity
ORIGINAL RESEARCH — Volume 16 — July 11, 2019

Seth A. Berkowitz, MD, MPH1,2; Sanjay Basu, MD, PhD3,4,5; Craig Gundersen, PhD6; Hilary K. Seligman, MD, MAS7,8 (View author affiliations)
Suggested citation for this article: Berkowitz SA, Basu S, Gundersen C, Seligman HK. State-Level and County-Level Estimates of Health Care Costs Associated with Food Insecurity. Prev Chronic Dis 2019;16:180549. DOI: http://dx.doi.org/10.5888/pcd16.180549.
PEER REVIEWED
On This Page
Summary
What is already known on this topic?
Food insecurity is associated with higher health care costs, on average.
What is added by this report?
We found substantial variation in state- and county-level health care expenditures associated with food insecurity. We also found that higher food insecurity prevalence is more strongly associated with higher spending than differences in health care prices or intensity of health care use.
What are the implications for public health practice?
A multi-level strategy that encompasses both area-level determinants of food insecurity (eg, local labor market factors and state-earned income tax credits) and hunger safety net programs may improve public health.
Abstract
Introduction
Food insecurity, or uncertain access to food because of limited financial resources, is associated with higher health care expenditures. However, both food insecurity prevalence and health care spending vary widely in the United States. To inform public policy, we estimated state-level and county-level health care expenditures associated with food insecurity.
Methods
We used linked 2011–2013 National Health Interview Survey/Medical Expenditure Panel Survey data (NHIS/MEPS) data to estimate average health care costs associated with food insecurity, Map the Meal Gap data to estimate state-level and county-level food insecurity prevalence (current though 2016), and Dartmouth Atlas of Health Care data to account for local variation in health care prices and intensity of use. We used targeted maximum likelihood estimation to estimate health care costs associated with food insecurity, separately for adults and children, adjusting for sociodemographic characteristics.
Results
Among NHIS/MEPS participants, 10,054 adults and 3,871 children met inclusion criteria. Model estimates indicated that food insecure adults had annual health care expenditures that were $1,834 (95% confidence interval [CI], $1,073–$2,595, P < .001) higher than food secure adults. For children, estimates were $80 higher, but this finding was not significant (95% CI, −$171 to $329, P = .53). The median annual health care cost associated with food insecurity was $687,041,000 (25th percentile, $239,675,000; 75th percentile, $1,140,291,000). The median annual county-level health care cost associated with food insecurity was $4,433,000 (25th percentile, $1,774,000; 75th percentile, $11,267,000). Cost variability was related primarily to food insecurity prevalence.
Conclusions
Health care expenditures associated with food insecurity vary substantially across states and counties. Food insecurity policies may be important mechanisms to contain health care expenditures.
Introduction
Food insecurity, or uncertain access to food because of limited financial resources, affected 12.9% of Americans in 2016 — more than 40 million individuals (1). Food insecurity is associated with numerous chronic health conditions, including diabetes mellitus, hypertension, coronary heart disease, chronic kidney disease, and depression (2–6). Perhaps for this reason, estimates from both the United States and Canada indicate that, on average, health care costs are substantially higher among food-insecure individuals than among food-secure individuals (7–9).
Although food insecure individuals in the United States experience higher health care costs on average, this average likely obscures substantial variation across states and counties. The Map the Meal Gap study (http://map.feedingamerica.org/) has shown that US food insecurity rates vary widely (10). Similarly, local pricing and intensity of health care use also differ in the United States, resulting in widespread variation in health care spending (11,12). Furthermore, these patterns do not necessarily match; an area with higher food insecurity may have lower health care prices, and vice versa. This means that estimating local health care costs associated with food insecurity is not straightforward.
Understanding variation in health care costs associated with food insecurity has substantial public health implications, because doing so can inform the implementation of new initiatives (eg, the Centers for Medicare & Medicaid Services’ Accountable Health Communities Model [13]) or state and local public health and nutrition programs. Such programs could focus scarce resources on areas where health care costs associated with food insecurity are high. Furthermore, local economic policy, particularly state-earned income tax credits, local wage conditions, and housing policies can influence food insecurity (14,15). Therefore, understanding variations in health care costs associated with food insecurity has implications beyond public health.
To help inform both policies and programs to address these issues, we sought to estimate county-level and state-level health care costs associated with food insecurity in the United States.
Methods
Study design and data sources
To generate local estimates of health care costs associated with food insecurity, we needed 3 key pieces of information: 1) the mean per-person dollar amount of excess health care expenditures among adults and children; 2) the number of food-insecure adults and children residing in each county and state; and 3) the variation, from the national average, in health care costs for each county and state. The rationale for this was that, because health care expenditures exhibit substantial geographic variability, a similar individual might have lower health care costs if they resided in a low-cost area (in terms of health care prices) and higher health care costs if they lived in a high-cost area, even if their health care needs were exactly the same. Because no single data source had information on all 3 of these factors, we needed to combine data from several sources to generate our estimates. The institutional review board at the University of North Carolina at Chapel Hill exempted this analysis of secondary data from human subjects review.
National Health Interview Survey/Medical Expenditure Panel Survey
To estimate the excess health care costs, if any, associated with food insecurity, we used linked data from the National Health Interview Survey (NHIS) (16) and the Medical Expenditure Panel Survey (MEPS) (17). NHIS is a nationally representative epidemiologic surveillance survey of the civilian noninstitutionalized US population (16). MEPS is a nationally representative cohort that collects detailed data on health care expenditures over a 2-year period and is drawn from NHIS participants (17). We used data collected from NHIS participants in 2011 who participated in MEPS during 2012–2013. We extracted information on the exposure of food security status from NHIS, which used a 10-item version of the United States Department of Agriculture food security survey module for adults with a 30-day look-back window (16). In accordance with standard scoring, raw scores of 0 to 2 were considered food secure and raw scores of 3 to 10 were considered food insecure (16). We used the MEPS total health care expenditures variable, which includes all health care costs (eg, inpatient admissions, outpatient visits, medication costs). Using NHIS food insecurity data and MEPS health care cost data ensures appropriate time ordering between the hypothesized exposure and outcome. More details on NHIS and MEPS data, as well as on the estimates and statistical methods used in this study, are provided at https://saberkowitz.web.unc.edu/supplemental-information/state-and-local-healthcare-costs/.
Map the Meal Gap
Data on the prevalence of food insecurity among adults and children at the county and state level came from Map the Meal Gap (MMG), which is based on US Census data (including the American Community Survey and Current Population Survey) and Bureau of Labor Statistics data. MMG methods have been published (10). MMG uses a 2-step process established by Feeding America to obtain estimates of food insecurity prevalence for all US counties. In the first step, the state-level determinants of food insecurity (for both children and adults) are estimated based on data from 2001 through 2016. The model components used are unemployment, poverty, median income, percentage Hispanic ethnicity, percentage African-American race, percentage living in owned housing, year fixed effects, and state fixed effects. These models are then used in the second step to produce food insecurity estimates at the county level, using county-specific variables. For our study, the county-specific variables were drawn from the 2016 American Community Survey 5-year estimates.
Dartmouth Atlas of Health Care
To estimate how a given county or state differed in health care spending (either based on prices or intensity of care) from the national average, we used data from the Dartmouth Atlas of Health Care (www.dartmouthatlas.org/), covering 2012–2013 because that was when cost data were collected, to calculate a “cost factor.” The resulting cost factor is greater than 1 for areas with higher-than-average costs and less than 1 for areas with lower-than-average costs (18).
Statistical analysis
Step 1 of our analysis was to determine national estimates of excess health care costs, if any, associated with food insecurity. To do this, we used NHIS and MEPS data. Analyses incorporated representativeness weights and survey design (clustering) information as appropriate. Because the mechanisms through which food insecurity may be associated with health care costs are likely different between adults and children, we stratified our data by age (≥18 years for adults and <18 years for children) and then made separate estimates in these groups. To generate the cost estimates, we drew on prior work examining the association between food insecurity and health care costs (8). Because health care cost data are notoriously difficult to analyze (19) and generalized linear models rely on certain assumptions that may not always be met in practice, we applied a targeted maximum likelihood estimation approach (TMLE). TMLE is a doubly robust analytic strategy that initially creates an estimate of the excess health care costs associated with food insecurity and then updates that estimate using a submodel that estimates the probability of being food insecure (20).
Using NHIS and MEPS data allowed us to estimate the mean per-person cost associated with food insecurity for adults and children, but NHIS and MEPS are not designed to estimate health care costs for every county or state. Therefore, in step 2, we multiplied our nationally representative per-person estimate of health care costs by the number of food insecure adults and children in each county and state (using data from MMG). Then, to account for county and state differences in health care spending, we multiplied by the cost factor for the locality. To bound the uncertainty in the estimates, we created a lower and upper bound by using the 95% confidence interval (CI) for the NHIS/MEPS estimate of average health care costs associated with food insecurity. Finally, we conducted correlation analyses to help understand whether local variations in health care costs associated with food insecurity are more closely related to food insecurity prevalence or local health care spending characteristics.
All dollar estimates were inflation adjusted to December 2016 dollars, following MEPS guidance (https://meps.ahrq.gov/about_meps/Price_Index.shtml). All analyses — with the exception of MMG estimates, which were derived using Stata version 14.2 (StataCorp LP) — were conducted in SAS version 9.4 (SAS Institute, Inc) and R version 3.4.2 (R Foundation).
Results
In the analyses of health care costs associated with food insecurity, 10,054 adults and 3,871 children were included. Both food-insecure adults and children were more likely than their food-secure counterparts to be racial/ethnic minorities, have lower income, and lack health insurance (Table 1).
In TMLE analyses that accounted for age, sex, race/ethnicity, income, education, health insurance, metropolitan residence, and region of residence within the country, model-based estimates showed that adults who were food insecure had annual health care expenditures that were $1,834 (95% CI, $1,073–$2,595) higher than adults who were food secure (P < .001). In children, the model-based estimate for health care costs associated with food insecurity was $80 annually, but this finding was not significant (P = 0.53, 95% CI, −$171 to $329). Among approximately 28,266,000 food-insecure adults and 12,938,000 food-insecure children in the United States in 2016, using these model-based point estimates of the excess cost associated with food insecurity translates to approximately $52.9 billion in excess health care expenditures associated with food insecurity in 2016 (95% CI, $31.8 billion to $74.3 billion). This represents 3% to 6% of the approximately $1.2 trillion in annual health care expenditures we estimate from MEPS data. Because the estimate for children was not significantly different from $0, taking only adult costs yielded a national estimate of $51.8 billion in excess health care expenditures in 2016 (95% CI, $31.7 billion to $74.2 billion).
Using the model-based estimates from our main analyses (eg, point estimate for adults of $1,834), we then calculated the costs associated with food insecurity for each state (including the District of Columbia) and county in the United States (Figures 1 and 2). Estimates by state are presented in Table 2 and estimates by county are presented in the Appendix. At the state level, adult food insecurity prevalence ranged from 6.8% (North Dakota) to 17.6% (Mississippi), and child food insecurity prevalence ranged from 10.3% (North Dakota) to 25.0% (New Mexico). At the state level, the mean annual model-based health care cost associated with food insecurity was $1,087,815,000 (standard deviation [SD], $1,407,496,000), and the median annual health care cost associated with food insecurity was $687,041,000 (25th percentile, $239,675,000; 75th percentile, $1,140,291,000). The state with the highest annual model-based health care cost associated with food insecurity was California, at $7,213,940,000, and the state with the lowest annual health care cost associated with food insecurity was North Dakota at $57,587,000. On a per capita basis, Mississippi had the highest health care cost associated with food insecurity, while North Dakota had the lowest. The 5 states with the highest per capita health care costs associated with food insecurity were Mississippi, Texas, Louisiana, Florida, and Oklahoma. The mean annual county-level health care cost associated with food insecurity was $17,905,000 (SD, $69,194,000), and the median annual county-level health care cost associated with food insecurity was $4,433,000 (25th percentile, $1,774,000; 75th percentile, $11,267,000).
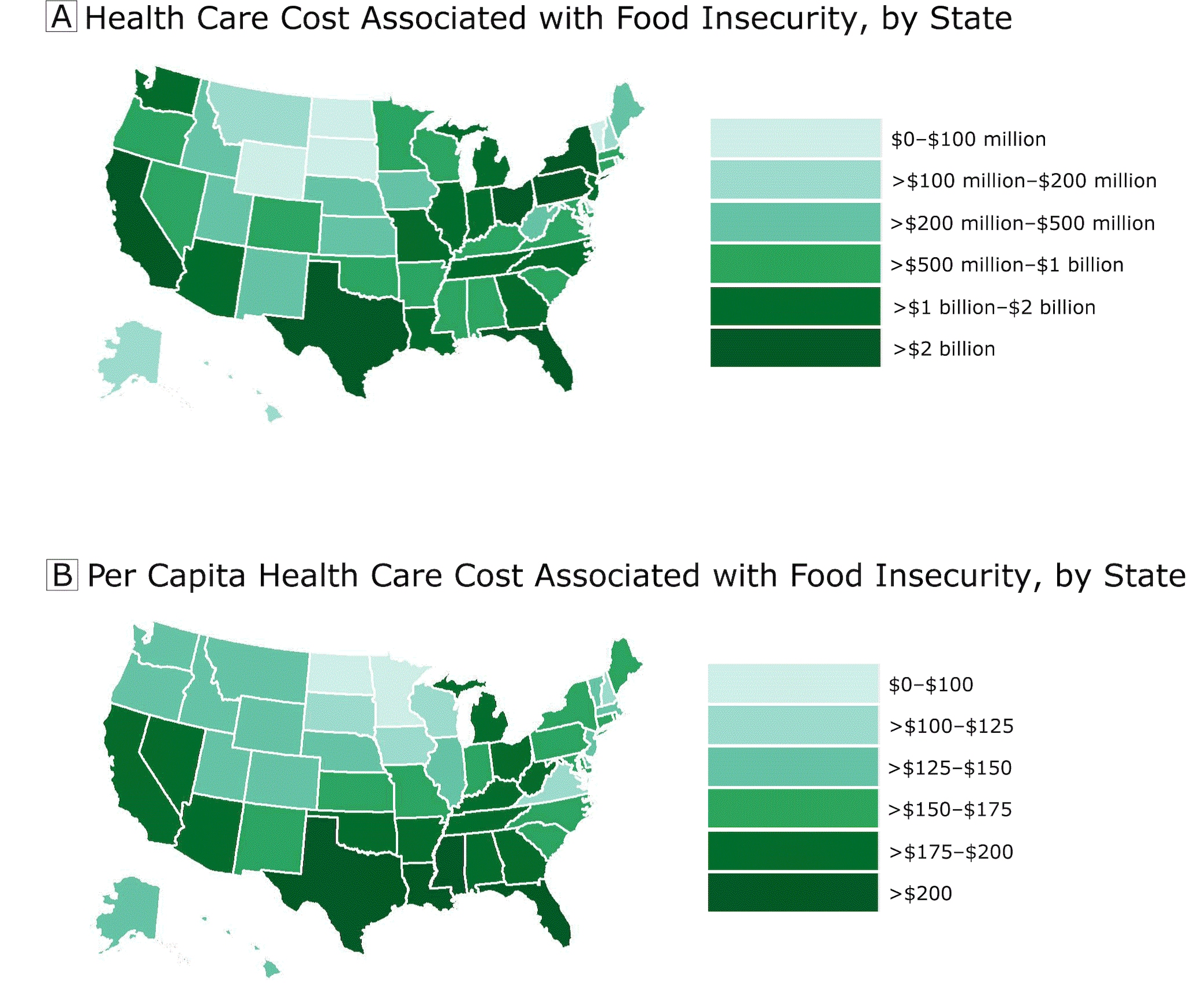
Figure 1.
Health care costs associated with food insecurity (A) and per capita health care costs associated with food insecurity (B), by state, United States, 2012–2013. [A text description of this figure is available.]
Health care costs associated with food insecurity (A) and per capita health care costs associated with food insecurity (B), by state, United States, 2012–2013. [A text description of this figure is available.]
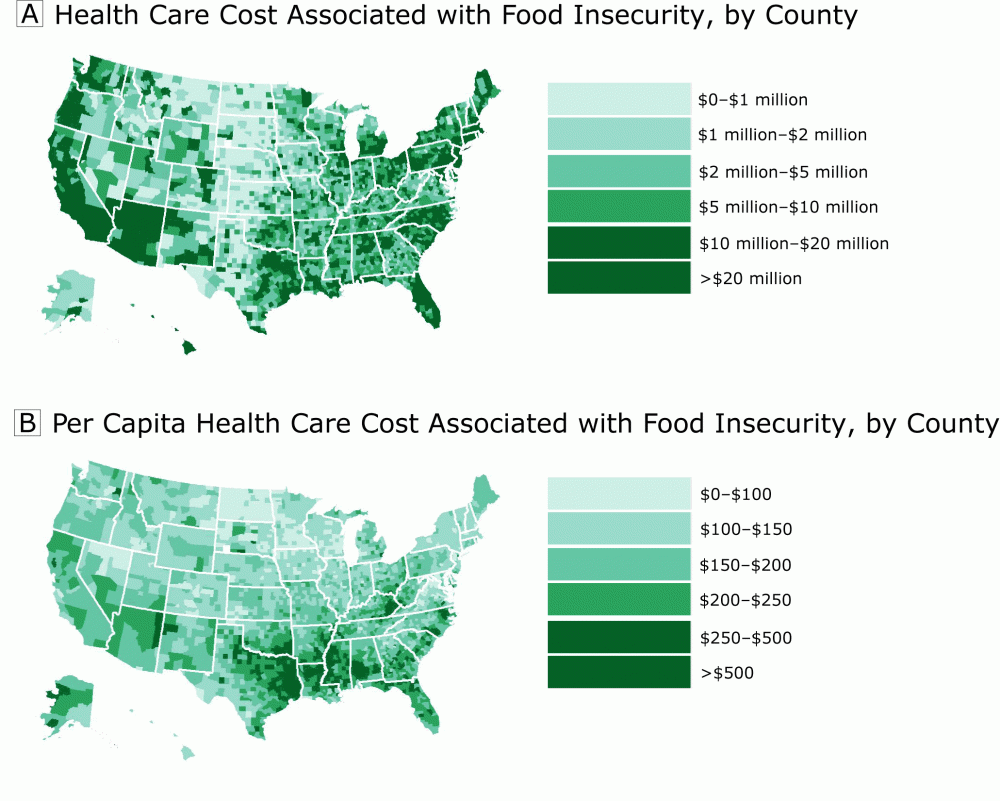
Figure 2.
Health care costs associated with food insecurity (A) and per capita health care costs associated with food insecurity (B), by county, United States, 2012–2013. [A text description of this figure is available.]
Health care costs associated with food insecurity (A) and per capita health care costs associated with food insecurity (B), by county, United States, 2012–2013. [A text description of this figure is available.]
The components of our cost estimates were the number of food-insecure individuals and the cost factor that accounted for local care intensity and prices. We found that at both the county and state level, the number of individuals who were food insecure was strongly correlated with the total expenditure estimate (r2 = 0.99 for county cost and r2 = 0.99 for state cost). The total expenditure estimate was only weakly or moderately associated with the cost factor (r2 = 0.22 for county cost and r2 = 0.57 for state cost). This suggests that a high proportion of the variation in food insecurity–associated health care expenditures is attributable to the number of food-insecure individuals.
Discussion
We found that food insecurity was associated with higher health care spending in adults and that this spending varied substantially across locality. Although patterns of local health care use and price explained some of this difference, the number of food-insecure individuals, and in particular the number of food-insecure adults, accounted for the largest share of variation in associated costs.
These findings are consistent with and expand our knowledge about the relationship between food insecurity and health care costs. Studies in both Canada (9) and the United States (7,8) have found that food insecurity is associated with higher health care costs. Specifically, a study from our research group (8) using similar methods found higher health care costs associated with food insecurity during a period when food insecurity prevalence was higher. Furthermore, recent research in the United States has found that, for several common clinical conditions, food insecurity is associated with excess health care costs even when accounting for other demographic and clinical characteristics (21). This may be related to several factors (2,22), including worse dietary quality in food-insecure individuals (23); trade-offs between food and other basics, such as medications, that make chronic disease management more difficult (24); and psychological factors, including stress and depressive symptoms (6). This study adds to this literature by quantifying the wide variation in excess expenditures. Although this study cannot determine why this variation occurs, the correlation analyses suggest that variation in model-based estimates of local health care costs associated with food insecurity is closely correlated with food insecurity prevalence in the area and less closely correlated with the local cost factor.
In our analyses, the point estimate for health care costs associated with food insecurity in children was small and not significantly different than $0. Although this study cannot determine why that is the case, past work suggests that food insecurity may be most closely related to increased health care cost through increased prevalence of chronic disease and exacerbation of those chronic conditions when they occur (8,22). If this is the case, then children may not see short-term (eg, the 2-year period in the NHIS/MEPS data) increases in health care costs simply because they are at low risk of developing these conditions, regardless of food security status. This does not imply, however, that food insecurity does not have long-term effects on children’s health or even short-term effects on important aspects of life that do not generate short-tern health care costs, like school achievement.
This study has implications for public health. Literature has demonstrated that local and state economic policies and conditions can have a substantial effect on food insecurity prevalence (14,15). In particular, lower tax burden (but not overall tax burden) for low-income individuals is associated with lower food insecurity, with strong associations between lower food insecurity and higher state-earned income tax credits (14,15). Other factors associated with lower food insecurity include local labor conditions and ease of access to hunger safety-net programs (14,15). For this reason, an important direction for future research will be to evaluate whether polices that reduce area food insecurity prevalence also lead to lower health care spending. Because there is evidence that individual-level nutrition interventions, particularly the Supplemental Nutrition Assistance Program (SNAP) (25–27) and medically tailored meal delivery programs (28), may also be associated with lower health care costs, having area-level policy options could provide a multilevel framework for addressing high health care spending by supporting access to proper nutrition. Fewer than 40% of individuals with food insecurity in this study had private health insurance, meaning that public health care programs, particularly at the state level, are shouldering much of the cost associated with food insecurity. SNAP and other nutrition programs are funded at the federal level, so if states worked to maximize uptake of federal nutrition programs, they may not only lower food insecurity rates but also decrease health care expenditures.
This study has several limitations. The costs estimated are likely conservative, because there is evidence that MEPS underestimates health care expenditures (29), and we did not consider indirect costs (like lost productivity owing to illness). Also, the sample used for estimating health care expenditures included only civilian noninstitutionalized individuals, which excludes some groups. The association between food insecurity and health care costs may not be fully related to food insecurity causing higher costs. There is likely to be a bidirectional relationship whereby food insecurity may worsen health, thus increasing health care costs, and worse health (and attendant expenses) may lead to food insecurity by decreasing the ability to work and increasing household debt. When examining the relationship between food insecurity and health care costs, there is a small delay between food security assessment in NHIS and the beginning of cost data collection in MEPS. Although assessment of food insecurity before collection of cost data is necessary to preserve time-ordering and mitigate reverse causation, the delay could lead to some misclassification (if food security status changes in the interval), which would tend to bias results to the null. Also, because NHIS and MEPS are not designed to yield county-level estimates of food insecurity prevalence or health care costs, we had to combine NHIS and MEPS data with data sources that were designed to provide more granular estimates. In addition, this is an inherently ecological analysis. However, since both the exposure (food insecurity prevalence) and the outcome (health care spending in the locality) were area-level assessments, this type of analysis is not subject to concerns about ecological fallacy (30). Finally, we did not have the ability to look at the specific distribution of comorbidities within each locality. To the extent that differences in comorbidities reflect differences in effect modifiers, actual local spending will not match the estimates. This would occur both for areas where individuals are less healthy than expected (and thus incur greater costs) and areas where individuals are healthier than expected (and correspondingly have lower health care costs).
Our study also has strengths. We used a nationally representative, longitudinal data set to estimate the association between food insecurity and health care costs. Furthermore, we used robust and well-validated methods to provide local estimates of food insecurity prevalence.
Food insecurity is associated with substantial health care expenditures, but there is evidence that this varies widely across states and counties. This variation suggests that local and state policies could be important mechanisms for improving health and containing health care expenditures. As health care cost containment remains a national priority, state and local strategies to reduce food insecurity rates may be an important public health tool.
Acknowledgments
The research reported in this publication was supported by Feeding America. The funders did not have any role in the conduct of the research or the decision to submit for publication. S.A.B. and S.B. have no conflicts of interest to report. Both C.G. and H.K.S. serve on Feeding America’s Technical Advisory Group. H.K.S. is also senior medical advisor at Feeding America. S.A.B.’s role in the research reported in this publication was also supported by the National Institute of Diabetes and Digestive and Kidney Diseases of the National Institutes of Health under award no. K23DK109200. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health.
Author Information
Corresponding Author: Seth A. Berkowitz, MD, MPH, 5034 Old Clinic Bldg, CB 7110, Chapel Hill, NC 27599. Telephone: 919-966-2276. Email: seth_berkowitz@med.unc.edu.
Author Affiliations: 1Division of General Medicine and Clinical Epidemiology, Department of Medicine, University of North Carolina at Chapel Hill School of Medicine, Chapel Hill, North Carolina. 2Cecil G. Sheps Center for Health Services Research, University of North Carolina at Chapel Hill, Chapel Hill, North Carolina. 3Research and Analytics, Collective Health, San Francisco, California. 4School of Public Health, Imperial College London, London, United Kingdom. 5Center for Primary Care, Harvard Medical School, Boston, Massachusetts. 6Department of Agricultural and Consumer Economics, University of Illinois, Urbana, Illinois. 7Departments of Medicine and Epidemiology and Biostatistics, University of California San Francisco, San Francisco, California. 8UCSF Center for Vulnerable Populations at Zuckerberg San Francisco General Hospital, San Francisco, California.
References
- Coleman-Jensen A, Rabbitt MP, Gregory CA, Singh A. Household food security in the United States in 2017. https://www.ers.usda.gov/publications/pub-details/?pubid=90022. Accessed September 25, 2018.
- Gundersen C, Ziliak JP. Food insecurity and health outcomes. Health Aff (Millwood) 2015;34(11):1830–9. CrossRef PubMed
- Berkowitz SA, Berkowitz TSZ, Meigs JB, Wexler DJ. Trends in food insecurity for adults with cardiometabolic disease in the United States: 2005-2012. PLoS One 2017;12(6):e0179172. CrossRef PubMed
- Seligman HK, Bindman AB, Vittinghoff E, Kanaya AM, Kushel MB. Food insecurity is associated with diabetes mellitus: results from the National Health and Nutrition Examination Survey (NHANES) 1999-2002. J Gen Intern Med 2007;22(7):1018–23. CrossRef PubMed
- Crews DC, Kuczmarski MF, Grubbs V, Hedgeman E, Shahinian VB, Evans MK, et al. ; Centers for Disease Control and Prevention Chronic Kidney Disease Surveillance Team. Effect of food insecurity on chronic kidney disease in lower-income Americans. Am J Nephrol 2014;39(1):27–35. CrossRef PubMed
- Leung CW, Epel ES, Willett WC, Rimm EB, Laraia BA. Household food insecurity is positively associated with depression among low-income supplemental nutrition assistance program participants and income-eligible nonparticipants. J Nutr 2015;145(3):622–7.CrossRef PubMed
- Berkowitz SA, Seligman HK, Meigs JB, Basu S. Food insecurity, health care utilization, and high cost: a longitudinal cohort study. Am J Manag Care 2018;24(9):399–404. PubMed
- Berkowitz SA, Basu S, Meigs JB, Seligman HK. Food insecurity and health care expenditures in the United States, 2011-2013. Health Serv Res 2017. PubMed
- Tarasuk V, Cheng J, de Oliveira C, Dachner N, Gundersen C, Kurdyak P. Association between household food insecurity and annual health care costs. CMAJ 2015;187(14):E429–36. CrossRef PubMed
- Gundersen C, Engelhard E, Waxman E. Map the meal gap: exploring food insecurity at the local level. Appl Econ Perspect Policy 2014;36(3):373–86. CrossRef
- Newhouse JP, Garber AM. Geographic variation in health care spending in the United States: insights from an Institute of Medicine report. JAMA 2013;310(12):1227–8. CrossRef PubMed
- Geographic variation in health care spending and promotion of high-value care. Institute of Medicine; 2018. http://www.nationalacademies.org/hmd/Activities/HealthServices/GeographicVariation.aspx. Accessed April 30, 2019.
- Alley DE, Asomugha CN, Conway PH, Sanghavi DM. Accountable health communities — addressing social needs through Medicare and Medicaid. N Engl J Med 2016;374(1):8–11. CrossRef PubMed
- Bartfeld J, Men F. Food insecurity among households with children: the role of the state economic and policy context. Soc Serv Rev 2017;91(4):691–732. CrossRef
- Bartfeld J, Dunifon R, Nord M, Carlson S. What factors account for state-to-state differences in food security? https://www.ers.usda.gov/publications/pub-details/?pubid=44133. Accessed April 30, 2019.
- Centers for Disease Control and Prevention. National Health Interview Survey; 2018. https://www.cdc.gov/nchs/nhis/index.htm. Accessed April 30, 2019.
- Agency for Healthcare Research and Quality. Medical Expenditure Panel Survey; 2018. https://meps.ahrq.gov/mepsweb/. Accessed April 30, 2019.
- The Dartmouth Institute. Dartmouth Atlas of Health Care; 2018. http://www.dartmouthatlas.org/tools/downloads.aspx. Accessed April 30, 2019.
- Manning WG, Mullahy J. Estimating log models: to transform or not to transform? J Health Econ 2001;20(4):461–94. CrossRefPubMed
- Schuler MS, Rose S. Targeted maximum likelihood estimation for causal inference in observational studies. Am J Epidemiol 2017;185(1):65–73. CrossRef PubMed
- Garcia SP, Haddix A, Barnett K. Incremental health care costs associated with food insecurity and chronic conditions among older adults. Prev Chronic Dis 2018;15:180058. CrossRef PubMed
- Seligman HK, Schillinger D. Hunger and socioeconomic disparities in chronic disease. N Engl J Med 2010;363(1):6–9. CrossRefPubMed
- Morales ME, Berkowitz SA. The relationship between food insecurity, dietary patterns, and obesity. Curr Nutr Rep 2016;5(1):54–60.CrossRef PubMed
- Berkowitz SA, Seligman HK, Choudhry NK. Treat or eat: food insecurity, cost-related medication underuse, and unmet needs. Am J Med 2014;127(4):303–310e3.
- Berkowitz SA, Seligman HK, Rigdon J, Meigs JB, Basu S. Supplemental Nutrition Assistance Program (SNAP) participation and health care expenditures among low-income adults. JAMA Intern Med 2017;177(11):1642–9. CrossRef PubMed
- Srinivasan M, Pooler JA. Cost-related medication nonadherence for older adults participating in SNAP, 2013–2015. Am J Public Health 2018;108(2):224–30. CrossRef PubMed
- Samuel LJ, Szanton SL, Cahill R, Wolff JL, Ong P, Zielinskie G, et al. Does the Supplemental Nutrition Assistance Program affect hospital utilization among older adults? The case of Maryland. Popul Health Manag 2017. PubMed
- Berkowitz SA, Terranova J, Hill C, Ajayi T, Linsky T, Tishler LW, et al. Meal delivery programs reduce the use of costly health care in dually eligible Medicare and Medicaid beneficiaries. Health Aff (Millwood) 2018;37(4):535–42. CrossRef PubMed
- Validating the collection of separately billed doctor expenditures for hospital services: results from the Medicare-MEPS Validation Study; 2018. https://meps.ahrq.gov/mepsweb/data_stats/Pub_ProdResults_Details.jsp?pt=Working+Paper&opt=2&id=855. Accessed April 30, 2019.
- Subramanian SV, Jones K, Kaddour A, Krieger N. Revisiting Robinson: the perils of individualistic and ecologic fallacy. Int J Epidemiol 2009;38(2):342–60, author reply 370–3. CrossRef PubMed
No hay comentarios:
Publicar un comentario