
Association Between Changes in Postpartum Weight and Waist Circumference and Changes in Cardiometabolic Risk Factors Among Women With Recent Gestational Diabetes
ORIGINAL RESEARCH — Volume 16 — April 18, 2019
Jacinda M. Nicklas, MD, MPH, MA1,2,3; Bernard A. Rosner, PhD4,5; Chloe A. Zera, MD, MPH6; Ellen W. Seely, MD1 (View author affiliations)
Suggested citation for this article: Nicklas JM, Rosner BA, Zera CA, Seely EW. Association Between Changes in Postpartum Weight and Waist Circumference and Changes in Cardiometabolic Risk Factors Among Women With Recent Gestational Diabetes. Prev Chronic Dis 2019;16:180308. DOI: http://dx.doi.org/10.5888/pcd16.180308.
PEER REVIEWED
Abstract
Introduction
Women with gestational diabetes mellitus (GDM) have a 30% to 70% risk for developing type 2 diabetes and are at increased risk for cardiovascular disease. Little is known about how anthropometric changes in the first postpartum year modify cardiometabolic risk factors.
Methods
We randomly assigned women in the Balance After Baby study to an intervention group consisting of participation in a web-based lifestyle program or to a control group in which no program was offered. We measured weight, height, waist circumference, blood pressure, lipids, insulin, adiponectin, interleukin-6, and high-sensitivity C-reactive protein, and we conducted 2-hour oral glucose tolerance tests at 6 weeks, 6 months, and 12 months postpartum. We evaluated whether women assigned to the intervention had improved cardiometabolic risk markers compared with the control group. We then conducted a post-hoc analysis, pooling the 2 groups to compare changes in weight and waist circumference with changes in cardiometabolic risk factors.
Results
Women in the intervention group did not significantly improve cardiometabolic risk markers compared with women in the control group. We noted a large overlap of weight change and change in waist circumference between groups. In our post-hoc analysis pooling groups, changes in diabetes and cardiovascular risk factors were significantly correlated with changes in weight and waist circumference. The strongest associations were observed for fasting insulin, HOMA, and fasting glucose.
Conclusion
Anthropometric changes in weight and waist circumference in women with recent GDM may affect cardiometabolic risk factors, even in the first postpartum year. Our study demonstrates the importance of the postpartum year as an opportunity to decrease future risk for diabetes and cardiovascular disease in women with a history of GDM.
Introduction
The incidence of gestational diabetes mellitus (GDM) in US women is from 3% to 9%, depending on the population and the diagnostic criteria used (1). The incidence of GDM has been rising with the increasing prevalence of overweight and obesity in the United States. Women with a history of GDM have an increased risk of developing type 2 diabetes (2), with a rapid increase in cumulative risk within the first 5 years postpartum (3) and an elevated risk sustained through 10 years postpartum (4). Type 2 diabetes is also a key risk factor for cardiovascular disease (CVD) in women because of its higher relative and absolute association with CVD in women compared with men (5). Studies show an increased 10-year CVD risk in women with GDM history (6), with evidence of earlier incidence of atherosclerosis (7) and a 26% increased risk of developing hypertension over 16 years (8).
In 2011 the American Heart Association published updated guidelines to include a history of GDM as a CVD risk factor when screening parous women (9), and they recommend surveillance and management of CVD risk factors in women with a history of GDM. Despite these risks, little prospective research has examined the effects of postpartum weight changes or changes in waist circumference on cardiometabolic risk following pregnancies complicated by GDM (10). Although several intervention trials have demonstrated significant reductions in weight among postpartum women with recent GDM, it is unclear how clinically significant the weight loss is, and they have not clearly demonstrated improvements in blood glucose levels or other cardiometabolic risk factors (11).
In the Balance after Baby study we adapted the Diabetes Prevention Program into a web-based lifestyle intervention designed to decrease postpartum weight retention in women with recent GDM (12). Women randomly assigned to the intervention group watched instructional videos, worked with a lifestyle coach, and were asked to track their weight and steps. In the analysis of the primary outcome, women assigned to the intervention group lost significantly more weight than women randomized to the control group (12). However, women randomly assigned to the intervention group did not demonstrate a significant improvement in glucose tolerance when compared with the control group, possibly because of the short follow-up period and small sample size (N = 75).
For this analysis we first sought to determine the effect of the web-based lifestyle intervention program on markers of cardiometabolic risk by analyzing the change by group assignment. Given the small sample size and substantial overlap in change in postpartum weight and waist circumference, we then pooled the sample to conduct post-hoc analyses to explore the effect of postpartum weight loss and changes in waist circumference on markers of cardiometabolic risk, irrespective of study group assignment. We sought to determine whether anthropometric changes in the first postpartum year were significantly associated with changes in cardiovascular, metabolic, and inflammatory markers.
Methods
Study population
The Balance after Baby randomized controlled trial (no. NCT01158131) was a prospective intervention study of 75 women with recent GDM to examine the effect of a web-based lifestyle intervention on postpartum weight loss. Feasibility and efficacy of the trial have been reported (12). Briefly, 75 postpartum women were studied in the first year after a pregnancy complicated by GDM. The study was conducted at Brigham and Women’s Hospital in Boston, Massachusetts, from June 2010 through September 2012. Inclusion criteria were being aged 18 to 45; having a diagnosis of GDM in the most recent pregnancy, according to Carpenter-Coustan criteria (13) or by documented clinical diagnosis in the medical record; and having a body mass index (BMI, kg/m2) of 24 or higher (≥22 for Asian participants) and less than 50. Women were excluded if they had a history of type 2 diabetes or bariatric surgery or if they were taking medications known to affect glucose metabolism or weight. Women were also excluded if they delivered before 32 weeks gestation or if they had net weight loss during pregnancy.
Qualifying participants attended an initial study visit at approximately 6 weeks postpartum for baseline measurements, and measures conducted at baseline were repeated at approximately 6 months and approximately 12 months postpartum. Women diagnosed with type 2 diabetes (by 2 abnormal oral glucose tolerance test [OGTT] values or a single abnormal value repeated and again found to be abnormal) at the 6-month visit completed the 12-month study visit excluding the OGTT. For the pooled analysis, we restricted the sample to women who had baseline measurements of anthropometry, blood pressure, and biomarkers, as well as anthropometric measurements, blood pressure, and a fasting blood sample at 6 months and/or 12 months.
Measurements
We measured weight, height, and waist circumference, and we also measured markers of cardiometabolic risk: hemoglobin A1c (HbA1c), fasting glucose, 75 g 2-hour OGTTs, fasting insulin, adiponectin, low-density lipoprotein (LDL) cholesterol, high-density lipoprotein (HDL) cholesterol, fasting triglycerides, blood pressure, and the inflammatory markers high-sensitivity C-reactive protein (hsCRP) and interleukin-6 (IL-6). We requested that women not perform exercise nor breastfeed during the OGTT. We calculated BMI and HOMA-IR ([fasting glucose × fasting insulin)/405).
Statistical analysis
We compared baseline characteristics using t tests or Wilcoxon rank sum tests for continuous variables and Pearson’s χ2 or Fisher’s exact tests for categorical variables. We calculated means for data that were normally distributed and medians for skewed data. Women who became pregnant, started assisted reproductive treatment, or had a neonatal death were censored at the time of these events. We estimated mixed-effects regression models using a random intercept and an unstructured covariance matrix to look at the effect of group assignment on change in markers of cardiometabolic risk in the intent-to-treat sample (n = 75). We controlled for baseline values of the cardiometabolic risk factors in the mixed-effects regression models. Data after censoring events were considered missing at random, except that we carried forward blood glucose and HbA1c values for 2 women who were diagnosed with type 2 diabetes at 6 months. As a sensitivity analysis, we estimated the mixed-effects regression models while controlling for breastfeeding status. For the post-hoc analysis of the pooled sample, we estimated regression models to assess the effect of changes in weight and waist circumference on markers of cardiometabolic risk. We controlled for differences at baseline by including the variable for the risk factor at the baseline visit in each model. We conducted a sensitivity analysis, controlling for breastfeeding status in each model. We used JMP 12–13 Pro SAS statistical software and SAS version 9.0 to conduct analyses (SAS Institute, Inc).
Results
Participants had a mean age of 33 years and a mean baseline postpartum BMI of 31 (Table 1). Fifty-seven percent were white, 31% were African American, 12% were Asian, and 20% identified as Hispanic. The only significant difference in characteristics between the intervention and control groups at baseline was diastolic blood pressure.
Women assigned to the intervention group had lost significantly more weight than those assigned to the control group at 6 months (−2.6 kg [95% confidence interval (CI), −4.4 to −0.8] vs 1.4 kg [95% CI, −0.4 to 3.1]; P = .003) and at 12 months (−2.8 kg [95% CI, −4.8 to −0.7] vs 0.5 kg [95% CI, −1.4 to 2.4]; P = .02 for difference between groups) (Table 2). We noted overlap in the intervention and control groups for both change in weight (−15.9 kg to 9.6 kg) and change in waist circumference (−30.6 cm to 14.5 cm) (Figure 1). The women assigned to the intervention group also had a significant decrease in BMI compared with the control group. Similarly, women in the intervention group were closer to their prepregnancy weight (−0.7 kg; 95% CI, −3.5 to 2.2) than women in the control group (4.0 kg, 95% CI, 1.3 to 6.8). More women in the intervention group with measured weights (11 of 28, 39%) compared with the control group (7 of 32, 22%) achieved weight loss of greater than or equal to 5%.
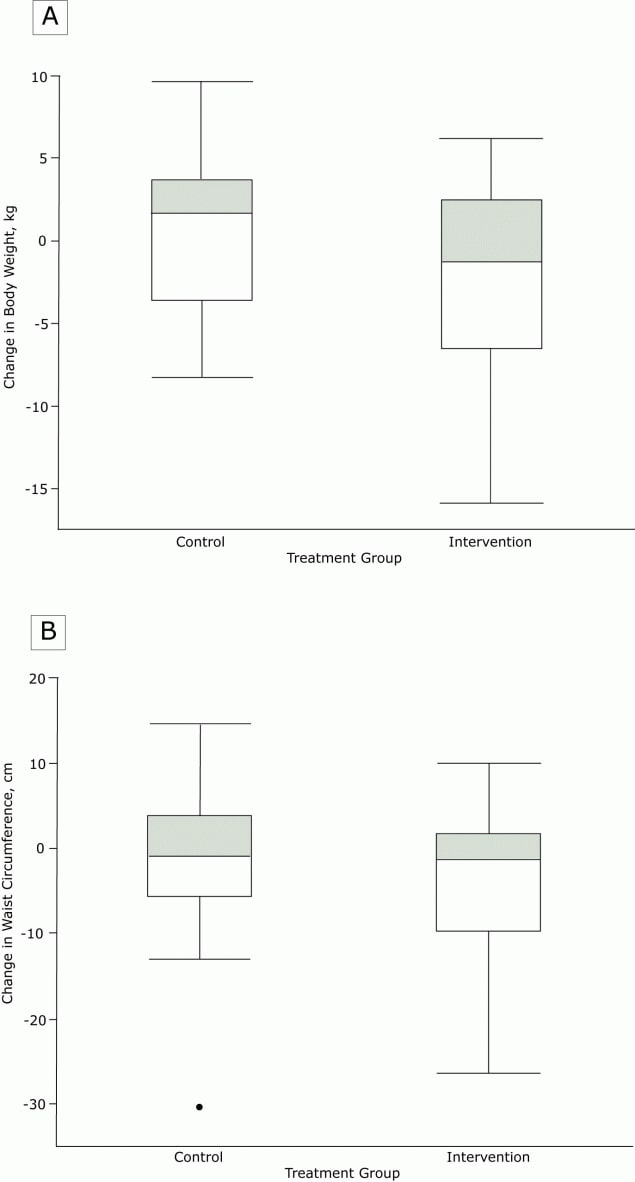
Figure 1.
Distribution of change in a) weight and b) waist circumference in the control and intervention groups at 12 months postpartum. [A text description of this figure is available.]
Distribution of change in a) weight and b) waist circumference in the control and intervention groups at 12 months postpartum. [A text description of this figure is available.]
Figure 1a shows the distribution of the change in body weight in the control and intervention groups at 12 months postpartum. There was substantial overlap in the interquartile range (−3.6 to 3.7 kg in the control group vs −6.6 to 2.4 kg in the intervention group). Figure 1b shows the distribution of the change in waist circumference in the control and intervention groups at 12 months postpartum. There was substantial overlap in the interquartile range (−5.8 to 3.8 cm in the control group vs −10.1 to 1.4 cm in the intervention group).
We observed no significant difference in change in waist circumference between women assigned to the intervention group and women assigned to the control group, although it trended in the same direction as weight and BMI at both 6 and 12 months. Overall fasting insulin and HOMA-IR tended to increase over time in both groups, and fasting lipids decreased over time in both groups. HsCRP also decreased in both groups over time. In the sensitivity analysis, including a variable in the mixed-effects regression models to represent breastfeeding status over time did not substantively change the findings.
In the pooled analysis, irrespective of group assignment, a positive change in weight was significantly associated with changes in most diabetes risk markers (Table 3). Some of the strongest relationships were seen for the change in fasting glucose and fasting insulin (Figure 2). The difference in mean fasting glucose between the tenth percentile of weight change and the 90th percentile of weight change in the entire cohort at 6 months (15.3 kg) was 12.5%. Over the 10th to 90th percentile range at 12 months (14.7 kg) it was 12.1% over the 12 month range. For fasting insulin, the change over the 10th to 90th percentile of weight change was 48% for 6 months and 58% at 12 months.
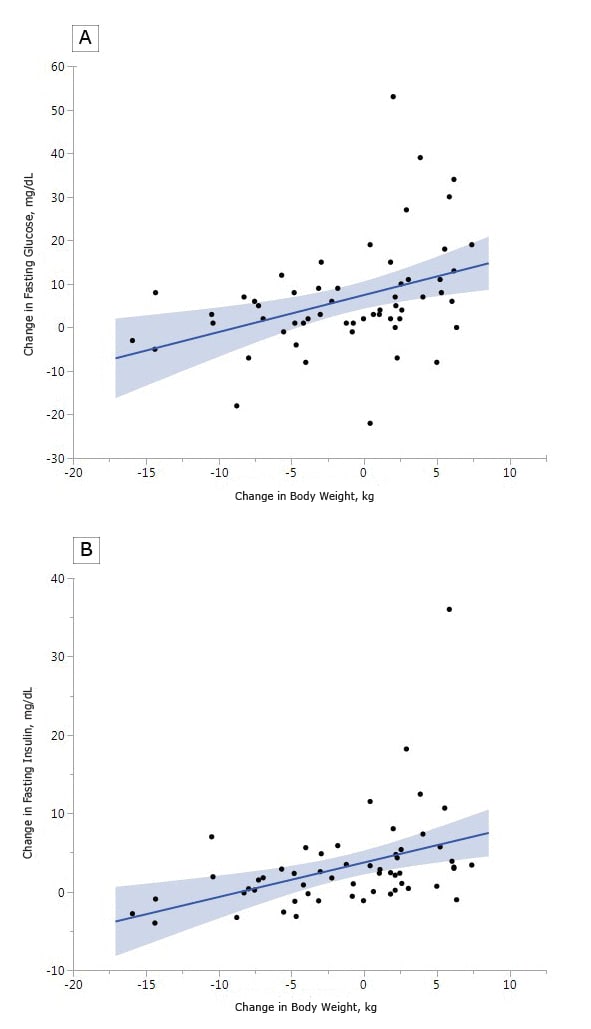
Figure 2.
Change in a) fasting glucose vs. change in weight at 12 months postpartum and b) fasting insulin and change in weight at 12 months postpartum. [A text description of this figure is available.]
Change in a) fasting glucose vs. change in weight at 12 months postpartum and b) fasting insulin and change in weight at 12 months postpartum. [A text description of this figure is available.]
Change in waist circumference was also significantly correlated with most diabetes risk markers, including fasting glucose and fasting insulin (Table 3). A change in triglycerides was significantly associated with weight change at both 6 and 12 months but not with change in waist circumference; hsCRP was significantly associated with both weight change and change in waist circumference at 12 months postpartum. None of the values changed significantly in sensitivity analyses when controlling for breastfeeding status. A substantial proportion of participants had 120-minute glucose values that were lower than their fasting glucose values (13% at 6 weeks, 9% at 6 months, and 24% at 12 months).
Discussion
We noted significant changes between the intervention and control groups for change in weight between baseline and 6 and 12 months postpartum, as well as the change from prepregnancy weight. In this population of women with recent GDM, a return to prepregnancy weight is clinically significant with respect to the prevention of type 2 diabetes and cardiovascular disease (12). However, women assigned to the intervention group did not have a significant improvement in markers of cardiometabolic risk when compared with the control group. This may have been because of the small sample size, the duration of the study, and the overlap in change in weight in both groups. In our post-hoc analysis in which the 2 groups were pooled, we noted that changes in diabetes and cardiovascular risk factors were significantly correlated with changes in both weight and waist circumference.
Overall, changes in weight were more often significantly correlated with cardiometabolic risk factors than changes in waist circumference. The strongest associations were seen for fasting insulin, HOMA, and fasting glucose. These findings illustrate that changes in weight and waist circumference in women with recent GDM have a significant relationship with diabetes risk factors, even in the first postpartum year. Although risk factors for cardiovascular disease had fewer significant correlations, significant relationships were noted between triglycerides and change in weight, as well as changes in weight and waist circumference and change in hsCRP.
Our findings demonstrated the strongest relationships between change in weight and markers of insulin sensitivity, including fasting glucose and insulin. The impact of weight loss on insulin sensitivity is well established. Studies demonstrate that postpartum insulin sensitivity is one of the strongest predictors of progression to type 2 diabetes following GDM in the first 5 years following the index pregnancy (14). Other studies looking at longer-term outcomes in women with prior GDM have shown the impact of weight changes on the incidence of type 2 diabetes. In one prospective cohort study of 1,695 women with a history of GDM, increases in weight and BMI were associated with increased risk of type 2 diabetes over 18 years of follow-up (15). Similarly, a retrospective cohort study of 1,263 Chinese women within 5 years of a GDM delivery demonstrated significantly increased risk for type 2 diabetes and prediabetes with weight gain and, conversely, decreased risk with weight loss (16). Post-hoc analyses of the Diabetes Prevention Program demonstrated that among older women who were on average 12 years away from their GDM pregnancy, women assigned to an intensive lifestyle program developed type 2 diabetes at a rate 50% lower than those women who had been assigned to the control group (17). These findings support recommendations in the literature suggesting that weight loss in the first postpartum year should delay or prevent onset of type 2 diabetes.
We did not find a significant association between 2-hour glucose and weight change in the pooled analysis. This may be because there was a substantial percentage of women with 2-hour glucose values lower than their baseline fasting glucose values. It has been hypothesized that these paradoxically low glucose values may be a precursor to insulin resistance (18). This may also be related to exercise, which was not objectively measured in this study.
Markers of cardiovascular risk have been less studied in the early postpartum period among women with a history of GDM. In one prospective study of 305 women, of whom approximately 30% had GDM, Kew and colleagues reported that women who gained weight between 3 and 12 months postpartum tended to have worsening of certain cardiometabolic risk factors, including blood pressure, HOMA-IR, adiponectin, and LDL cholesterol (19). They did not see differences in OGTT results, triglycerides, HDL cholesterol or hsCRP after adjustment for covariates, and they did not evaluate changes in waist circumference. Given that the adverse metabolic profiles were largely not apparent at 3 months but emerged at 12 months, the authors suggested increased focus on the postpartum year for limiting postpartum weight retention (19) through interventions and increasing physical activity. In our study we saw a pronounced decrease in both lipids and hsCRP from baseline to 12 months. Lipid levels are known to increase during pregnancy and return to baseline postpartum (20). In our study, among cardiovascular risk factors, only triglycerides demonstrated a significant relationship with weight changes in the postpartum year. Study findings are mixed for hsCRP levels in pregnancy and postpartum; some showed an increase through pregnancy and postpartum and others demonstrated a decrease. Studies demonstrated larger increases among obese women (21,22). In our study, we noted an expected decrease in hsCRP overall postpartum, and a significant relationship with changes in weight at 12 months.
Fewer data are available on the relationship between changes in waist circumference and cardiometabolic risk factors. Among studies in general populations, findings are mixed on whether changes in weight or waist circumference are a more powerful predictor of changes in cardiometabolic risk factors (23–26). Although decreases in waist circumference improve triglycerides, blood pressure, and hyperglycemia in nonpostpartum populations (27), little is known about these changes in the postpartum period. Given the changes in waist circumference related to childbearing as well as parity, the relationship between changes in waist circumference and cardiometabolic risk factors may be more difficult to characterize. Several studies have demonstrated that postpartum weight retention tends to be more centrally distributed, which likely increases the likelihood of worsening cardiometabolic risk (28). One long-term study (28) with a mean follow-up of 7.3 years noted that postpartum increases in weight and waist circumference among Finnish women with GDM during pregnancy predicted the development of hyperglycemic conditions (10).
Limitations of this study include its being a single-site study with a small sample size and the use of multiple correlations to analyze the relationships between weight change and cardiometabolic markers. The pooled analysis was a post-hoc analysis and therefore should be considered hypothesis-generating. Our data set also contained missing values at some points.
Studies show that pregnancy weight retained beyond 6 to 12 months postpartum is more likely to be retained long-term and is a powerful independent risk factor for future obesity (29), which has prompted calls for decreasing postpartum weight retention. The findings from our analysis provide further justification for early postpartum weight loss and the reduction of waist circumference given the association with changes in cardiometabolic risk factors even during this first year after delivery. Our study adds further evidence to the potential for the postpartum year to serve as a window of opportunity to decrease future risk of obesity and chronic disease (30), particularly diabetes. Future studies should also examine how changes in these cardiometabolic risk factors relate to the acquisition of diabetes and cardiovascular disease in subsequent years.
Acknowledgments
The authors thank the women who participated in the Balance after Baby randomized trial, and the Clinical and Informatics cores of the Harvard Clinical and Translational Science Award for providing nursing and laboratory services. We thank Suzette Bossart and Danielle Cook for their assistance with manuscript preparation.
The Balance after Baby study was supported by the Centers for Disease Control and Prevention (CDC MM-1094-09/09), and work by the investigators was supported by an Institutional National Research Service Award no. T32AT000051 from the National Center for Complementary and Alternative Medicine (NCCAM) at the National Institutes of Health, an NIH BIRCWH K12 HD057022, a K24 from the National Heart, Lung, and Blood Institute at the National Institutes of Health (9K24HL096141), and a K23 from the National Heart, Lung, and Blood Institute at the National Institutes of Health (1K23HL133604-01). The findings and conclusions are those of the authors and do not necessarily represent the official position of the Centers for Disease Control and Prevention. Copyrighted material was not used. No copyrighted surveys, instruments, or tools were used.
Author Information
Corresponding Author: Jacinda M. Nicklas, MD, MPH, MA, Division of General Internal Medicine, University of Colorado School of Medicine, Aurora, CO 80045. Telephone: 303-724-9028. Email: Jacinda.Nicklas@ucdenver.edu.
Author Affiliations: 1Division of Endocrinology, Diabetes and Hypertension, Brigham and Women’s Hospital, Boston, Massachusetts. 2Division of General Medicine and Primary Care, Beth Israel Deaconess Medical Center, Boston, Massachusetts. 3Division of General Internal Medicine, University of Colorado School of Medicine, Aurora, Colorado. 4Channing Division of Network Medicine, Department of Medicine, Harvard Medical School, Boston, Massachusetts. 5Department of Biostatistics, Harvard School of Public Health, Boston, Massachusetts. 6Division of Maternal-Fetal Medicine, Department of Obstetrics and Gynecology, Brigham and Women’s Hospital Boston, Massachusetts.
References
- DeSisto CL, Kim SY, Sharma AJ. Prevalence estimates of gestational diabetes mellitus in the United States, Pregnancy Risk Assessment Monitoring System (PRAMS), 2007–2010. Prev Chron Dis 2014;11.
- Bellamy L, Casas JP, Hingorani AD, Williams D. Type 2 diabetes mellitus after gestational diabetes: a systematic review and meta-analysis. Lancet 2009;373(9677):1773–9. CrossRefPubMed
- Kim C, Newton KM, Knopp RH. Gestational diabetes and the incidence of type 2 diabetes: a systematic review. Diabetes Care 2002;25(10):1862–8.
- Aroda VR, Edelstein SL, Zhang P, Herman WH, Barrett-Connor E, Delahanty LM, et al. ; Diabetes Prevention Program Research Group. The effect of lifestyle intervention and metformin on preventing or delaying diabetes among women with and without gestational diabetes: the Diabetes Prevention Program Outcomes Study 10-year follow-up. JCEM 2015.
- Sarwar N, Gao P, Seshasai SR, Gobin R, Kaptoge S, Di Angelantonio E, et al. Diabetes mellitus, fasting blood glucose concentration, and risk of vascular disease: a collaborative meta-analysis of 102 prospective studies. Lancet 2010;375(9733):2215–22. Erratum in: Lancet 2010;376(9745):958. PubMed https://doi.org/10.1016/S0140-6736(10)60484-9
- Retnakaran R, Hanley AJ, Raif N, Connelly PW, Sermer M, Zinman B. C-reactive protein and gestational diabetes: the central role of maternal obesity. J Clin Endocrinol Metab 2003;88(8):3507–12. CrossRef PubMed
- Gunderson EP, Chiang V, Pletcher MJ, Jacobs DR Jr, Quesenberry CP Jr, Sidney S, et al. History of gestational diabetes mellitus and future risk of atherosclerosis in mid-life: the Coronary Artery Risk Development in Young Adults study. J Am Heart Assoc 2014;3(2):e000490. CrossRef PubMed
- Tobias DK, Hu FB, Forman JP, Chavarro J, Zhang C. Increased risk of hypertension after gestational diabetes mellitus: findings from a large prospective cohort study. Diabetes Care 2011;34(7):1582–4. CrossRef PubMed
- Mosca L, Benjamin EJ, Berra K, Bezanson JL, Dolor RJ, Lloyd-Jones DM, et al. Effectiveness-based guidelines for the prevention of cardiovascular disease in women — 2011 update: a guideline from the American Heart Association. Circulation 2011;123(11):1243–62. CrossRef PubMed
- Huopio H, Hakkarainen H, Pääkkönen M, Kuulasmaa T, Voutilainen R, Heinonen S, et al. Long-term changes in glucose metabolism after gestational diabetes: a double cohort study. BMC Pregnancy Childbirth 2014;14(1):296. CrossRef PubMed
- Di Cianni G, Lacaria E, Lencioni C, Resi V. Preventing type 2 diabetes and cardiovascular disease in women with gestational diabetes — The evidence and potential strategies. Diabetes Res Clin Pract 2018;145:184–92. CrossRef PubMed
- Nicklas JM, Zera CA, England LJ, Rosner BA, Horton E, Levkoff SE, et al. A web-based lifestyle intervention for women with recent gestational diabetes mellitus: a randomized controlled trial. Obstet Gynecol 2014;124(3):563–70. CrossRef PubMed
- Carpenter MW, Coustan DR. Criteria for screening tests for gestational diabetes. Am J Obstet Gynecol 1982;144(7):768–73. CrossRef PubMed
- Metzger BE, Cho NH, Roston SM, Radvany R. Prepregnancy weight and antepartum insulin secretion predict glucose tolerance five years after gestational diabetes mellitus. Diabetes Care 1993;16(12):1598–605. CrossRef PubMed
- Bao W, Yeung E, Tobias DK, Hu FB, Vaag AA, Chavarro JE, et al. Long-term risk of type 2 diabetes mellitus in relation to BMI and weight change among women with a history of gestational diabetes mellitus: a prospective cohort study. Diabetologia 2015;58(6):1212–9. CrossRef PubMed
- Li W, Liu H, Qiao Y, Lv F, Zhang S, Wang L, et al. Metabolic syndrome of weight change from pre-pregnancy to 1–5 years post-partum among Chinese women with prior gestational diabetes. Diabet Med 2015;32(11):1492–9. CrossRef PubMed
- Ratner RE CC, Metzger BE, Dabelea D, Bennett PH, Pi-Sunyer X, Fowler S, Kahn SE. Diabetes Prevention Program Research Group. Prevention of diabetes in women with a history of gestational diabetes: effects of metformin and lifestyle interventions. J Clin Endocrinol Metab 2008;93(12):4774–9.
- Guiducci L, Iervasi G, Quinones-Galvan A. On the paradox insulin resistance/insulin hypersensitivity and obesity: two tales of the same history. Expert Rev Cardiovasc Ther 2014;12(6):637–42. CrossRef PubMed
- Kew S, Ye C, Hanley AJ, Connelly PW, Sermer M, Zinman B, et al. Cardiometabolic implications of postpartum weight changes in the first year after delivery. Diabetes Care 2014;37(7):1998–2006. CrossRef PubMed
- Stuebe AM, Rich-Edwards JW. The reset hypothesis: lactation and maternal metabolism. Am J Perinatol 2009;26(1):81–8. CrossRef PubMed
- Pendeloski KPT, Ono E, Torloni MR, Mattar R, Daher S. Maternal obesity and inflammatory mediators: a controversial association. Am J Reprod Immunol 2017;77(5):e12674. CrossRefPubMed
- Christian LM, Porter K. Longitudinal changes in serum proinflammatory markers across pregnancy and postpartum: effects of maternal body mass index. Cytokine 2014;70(2):134–40. CrossRef PubMed
- Gautier A, Roussel R, Ducluzeau PH, Lange C, Vol S, Balkau B, et al. ; DESIR Study Group. Increases in waist circumference and weight as predictors of type 2 diabetes in individuals with impaired fasting glucose: influence of baseline BMI: data from the DESIR study. Diabetes Care 2010;33(8):1850–2. CrossRef PubMed
- Koh-Banerjee P, Wang Y, Hu FB, Spiegelman D, Willett WC, Rimm EB. Changes in body weight and body fat distribution as risk factors for clinical diabetes in US men. Am J Epidemiol 2004;159(12):1150–9. CrossRef PubMed
- Williams PT. Changes in body weight and waist circumference affect incident hypercholesterolemia during 7 years of follow-up. Obesity (Silver Spring) 2008;16(9):2163–8. CrossRefPubMed
- Nicklas JM, Sacks FM, Smith SR, LeBoff MS, Rood JC, Bray GA, et al. Effect of dietary composition of weight loss diets on high-sensitivity C-reactive protein: the Randomized POUNDS LOST trial. Obesity (Silver Spring) 2013;21(4):681–9. CrossRef PubMed
- Fanghänel G, Sánchez-Reyes L, Félix-García L, Violante-Ortiz R, Campos-Franco E, Alcocer LA. Impact of waist circumference reduction on cardiovascular risk in treated obese subjects. Cir Cir 2011;79(2):175–81. PubMed
- Gunderson EP, Murtaugh MA, Lewis CE, Quesenberry CP, West DS, Sidney S. Excess gains in weight and waist circumference associated with childbearing: the Coronary Artery Risk Development in Young Adults study (CARDIA). Int J Obes Relat Metab Disord 2004;28(4):525–35. CrossRef PubMed
- Rooney BL, Schauberger CW. Excess pregnancy weight gain and long-term obesity: one decade later. Obstet Gynecol 2002;100(2):245–52. CrossRef PubMed
- Rich-Edwards JW, Fraser A, Lawlor DA, Catov JM. Pregnancy characteristics and women’s future cardiovascular health: an underused opportunity to improve women’s health? Epidemiol Rev 2014;36(1):57–70. CrossRef PubMed






















.png)








No hay comentarios:
Publicar un comentario