01/21/2014 08:41 PM EST
Source: National Center for Health Statistics
Related MedlinePlus Page: Personal Health Records
Related MedlinePlus Page: Personal Health Records
NCHS Data Brief
Number 143, January 2014
Use and Characteristics of Electronic Health Record Systems Among Office-based Physician Practices: United States, 2001–2013
PDF Version  (621 KB)
(621 KB)
(621 KB)Chun-Ju Hsiao, Ph.D., and Esther Hing, M.P.H.
Key findings
- In 2013, 78% of office-based physicians used any type of electronic health record (EHR) system, up from 18% in 2001.
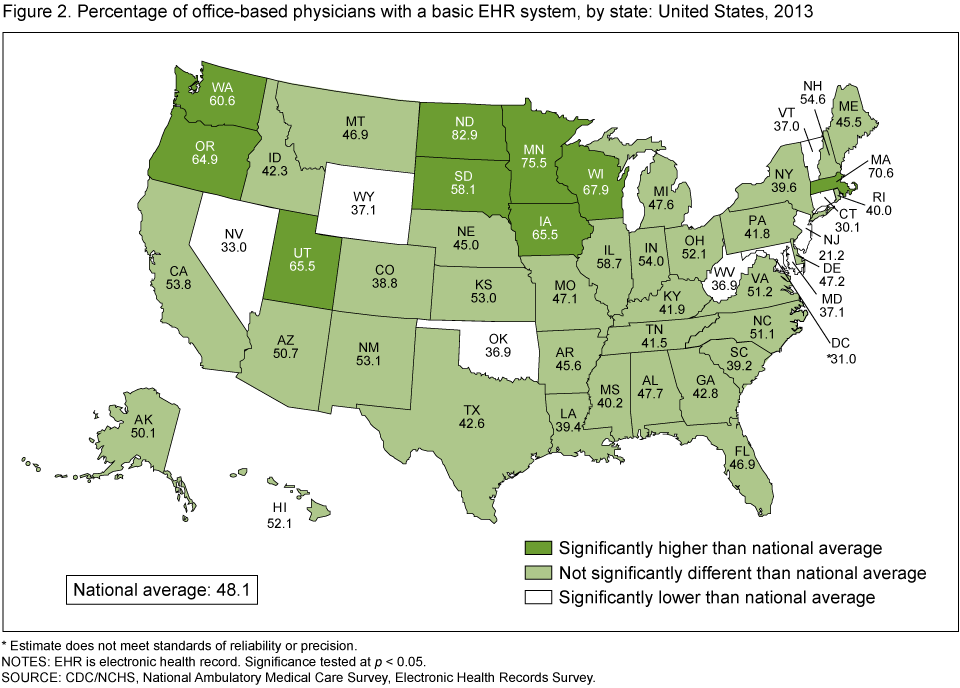
- In 2013, 48% of office-based physicians reported having a system that met the criteria for a basic system, up from 11% in 2006. The percentage of physicians with basic systems by state ranged from 21% in New Jersey to 83% in North Dakota.
- In 2013, 69% of office-based physicians reported that they intended to participate (i.e., they planned to apply or already had applied) in "meaningful use" incentives. About 13% of all office-based physicians reported that they both intended to participate in meaningful use incentives and had EHR systems with the capabilities to support 14 of the Stage 2 Core Set objectives for meaningful use.
- From 2010 (the earliest year that trend data are available) to 2013, physician adoption of EHRs able to support various Stage 2 meaningful use objectives increased significantly.
The Health Information Technology for Economic and Clinical Health (HITECH) Act of 2009 authorized incentive payments to increase physician adoption of electronic health record (EHR) systems (1,2). The Medicare and Medicaid EHR Incentive Programs are staged in three steps, with increasing requirements for participation. To receive an EHR incentive payment, physicians must show that they are "meaningfully using" certified EHRs by meeting certain objectives (3,4). This report describes trends in the adoption of EHR systems from 2001 through 2013, as well as physicians' intent to participate in the EHR Incentive Programs and their readiness to meet 14 of the Stage 2 Core Set objectives for meaningful use in 2013.
Keywords: health information technology, National Ambulatory Medical Care Survey
Adoption of basic EHR systems by office-based physicians increased 21% between 2012 and 2013.
- Use of any type of EHR system by office-based physicians increased from 18% in 2001 to 48% in 2009 and 78% in the 2013 estimates; 2009 is the year the HITECH Act authorized incentive payments to increase EHR adoption (Figure 1).
- In 2013, 48% of office-based physicians reported having a system that met the criteria for a basic system, up from 11% in 2006—the first year that information on basic systems is available.
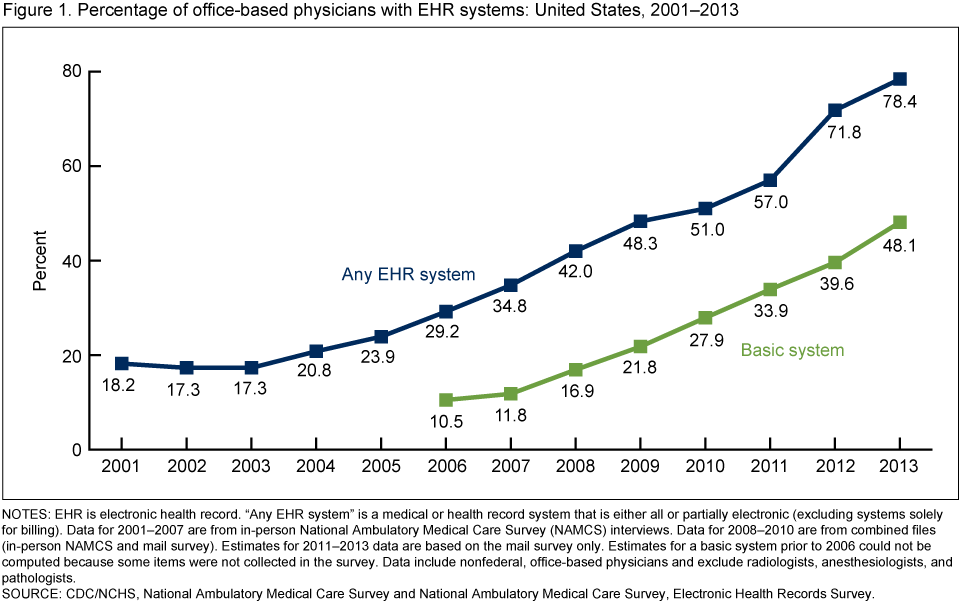
NOTES: EHR is electronic health record. “Any EHR system” is a medical or health record system that is either all or partially electronic (excluding systems solely for billing). Data for 2001–2007 are from in-person National Ambulatory Medical Care Survey (NAMCS) interviews. Data for 2008–2010 are from combined files (in-person NAMCS and mail survey). Estimates for 2011–2013 data are based on the mail survey only. Estimates for a basic system prior to 2006 could not be computed because some items were not collected in the survey. Data include nonfederal, office-based physicians and exclude radiologists, anesthesiologists, and pathologists.
SOURCE: CDC/NCHS, National Ambulatory Medical Care Survey and National Ambulatory Medical Care Survey, Electronic Health Records Survey.
SOURCE: CDC/NCHS, National Ambulatory Medical Care Survey and National Ambulatory Medical Care Survey, Electronic Health Records Survey.
Adoption of basic EHR systems and any EHR system varied widely across states.
- In 2013, the percentage of physicians who had a system meeting the criteria for a basic system ranged from 21% in New Jersey to 83% in North Dakota (Figure 2).
- The percentage of physicians who had a system meeting the criteria for a basic system was lower than the national average (48%) in eight states (Connecticut, Maryland, Nevada, New Jersey, Oklahoma, Vermont, West Virginia, and Wyoming) and higher than the national average in nine states (Iowa, Massachusetts, Minnesota, North Dakota, Oregon, South Dakota, Utah, Washington, and Wisconsin).
- In 2013, the percentage of physicians using any type of EHR system ranged from 66% in New Jersey to 94% in Minnesota (data not shown).
Figure 2. Percentage of office-based physicians with a basic EHR system, by state: United States, 2013
* Estimate does not meet standards of reliability or precision.
NOTES: EHR is electronic health record. Significance tested at p < 0.05.
SOURCE: CDC/NCHS, National Ambulatory Medical Care Survey, Electronic Health Records Survey.
NOTES: EHR is electronic health record. Significance tested at p < 0.05.
SOURCE: CDC/NCHS, National Ambulatory Medical Care Survey, Electronic Health Records Survey.
Sixty-nine percent of physicians intended to participate in the Medicare or Medicaid EHR Incentive Programs as of 2013.
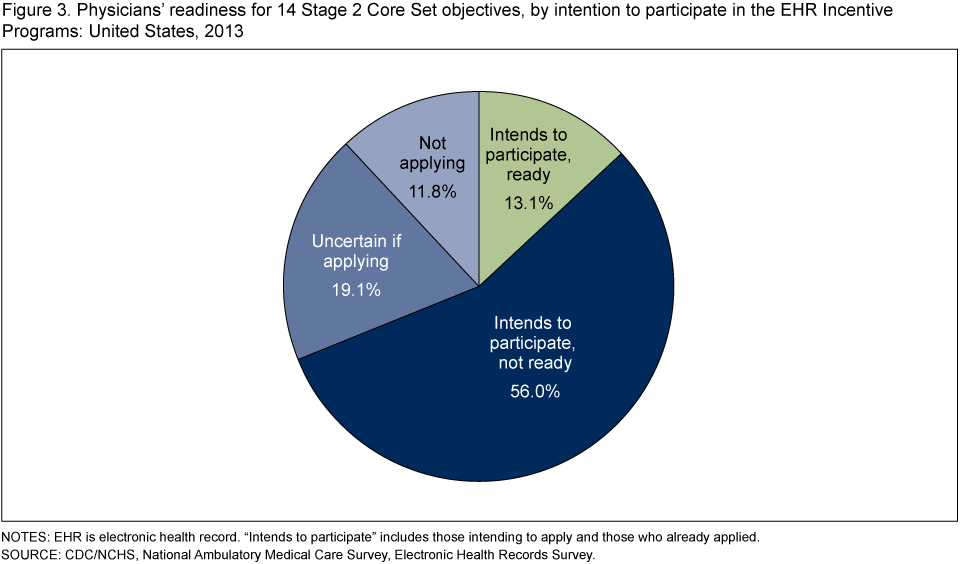
- In 2013, 69% of physicians intended to participate (i.e., they planned to apply or already had applied) in the Medicare or Medicaid Incentive Program, while 19% of physicians were uncertain and 12% were not going to apply (Figure 3). The percentage of physicians participating in either the Medicare or Medicaid Incentive Program increased 5% from 2012 (66%) to 2013 (69%) (5).
- About 13% of all office-based physicians reported that they both intended to participate in meaningful use incentives and had EHR systems with the capabilities to support 14 of the 17 Stage 2 Core Set objectives for meaningful use (see theTable for the 17 Stage 2 Core Set objectives).
- Of physicians intending to participate in the EHR Incentives Programs, 19% had EHR systems with the capabilities to support 14 of the 17 Stage 2 Core Set objectives for meaningful use.
- About 56% of all physicians intended to participate in the EHR Incentive Programs but did not have EHR systems with the capabilities to support 14 of the Stage 2 Core Set objectives for meaningful use. This percentage accounts for about four-fifths of physicians intending to participate in the EHR Incentive Programs (81%).
Figure 3. Physicians’ readiness for 14 Stage 2 Core Set objectives, by intention to participate in the EHR Incentive Programs: United States, 2013
NOTES: EHR is electronic health record. “Intends to participate” includes those intending to apply and those who already applied.
SOURCE: CDC/NCHS, National Ambulatory Medical Care Survey, Electronic Health Records Survey.
SOURCE: CDC/NCHS, National Ambulatory Medical Care Survey, Electronic Health Records Survey.
From 2010 through 2013, physician adoption of EHRs able to support seven Stage 2 meaningful use objectives for which 2010 data are available increased significantly.
- Increased adoption occurred for all seven of the capabilities for which trend data from 2010 are available. Adoption increased 12% for the objective recording patient demographics and increased 80% for the objective sending prescriptions electronically (calculated from Figure 4).
- In 2013, the adoption of computerized capabilities supporting seven Stage 2 Core objectives for meaningful use ranged from 39% (submitting electronic data to immunization registries or information systems) to 83% (recording patient demographics) (Figure 4).
Figure 4. Percentage of physicians with computerized capabilities to meet selected Stage 2 Core Set objectives: United States, 2010–2013
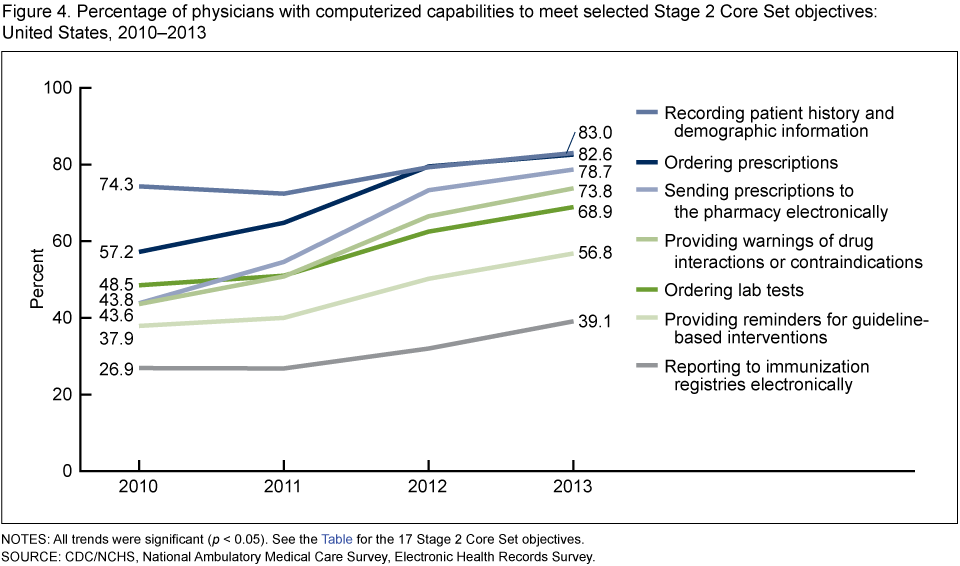
NOTES: All trends were significant (p < 0.05). See the Table for the 17 Stage 2 Core Set objectives.
SOURCE: CDC/NCHS, National Ambulatory Medical Care Survey, Electronic Health Records Survey.
SOURCE: CDC/NCHS, National Ambulatory Medical Care Survey, Electronic Health Records Survey.
Summary
In 2013, the National Ambulatory Medical Care Survey (NAMCS) EHR Survey showed that about 78% of office-based physicians used any EHR system. Since 2006 (first year for which data are available), the percentage of physicians who reported having an EHR system that met the criteria for a basic system increased 336%—from 11% in 2006 to 48% in 2013.
Adoption of a basic EHR system varied greatly by state. Adoption ranged from 21% in New Jersey to 83% in North Dakota.
To qualify for the Stage 2 meaningful use incentive in 2014, eligible physicians must meet all 17 of the Stage 2 Core objectives for meaningful use and 3 of the 6 Menu Set objectives, using certified EHR systems (3). In this report, estimates of physicians' readiness to meet meaningful use measures were limited to 14 of the 17 computerized capabilities that support the Stage 2 Core objectives.
In 2013, 69% of physicians reported intending to participate (having already applied or intending to apply) in the Medicare or Medicaid EHR Incentive Programs. However, only 13% of all physicians reported that they intended to participate in the EHR Incentive Programs and had an EHR system with the capabilities to support 14 of the 17 Stage 2 Core Set objectives for meaningful use. This may be an overestimate of the percentage meeting the Stage 2 requirements, because some physicians with systems supporting the 14 core objectives examined in this report may have a system that does not support the remaining 3 objectives, or 3 of the 6 Menu Set objectives required for payment.
From 2010 through 2013, physician adoption of 7 of the 17 capabilities required for Stage 2 Core objectives for meaningful use increased significantly. Computerized capabilities to send prescriptions to the pharmacy electronically and to provide warnings of drug interactions or contraindications had the largest increases.
Definitions
Physician office: A place where nonfederally employed physicians provide direct patient care in the 50 states and the District of Columbia; excludes radiologists, anesthesiologists, and pathologists.
Any EHR system: Obtained from "yes" responses to the question, "Does this practice use electronic medical records or electronic health records (not including billing records)?" In this report, "yes" responses are reported as having any EHR system. In recent years, the terms "electronic medical record" and EHR have been used interchangeably.
Basic EHR system: A system that has all of the following functionalities: patient history and demographics, patient problem lists, physician clinical notes, comprehensive list of patients' medications and allergies, computerized orders for prescriptions, and ability to view laboratory and imaging results electronically (6). Having a comprehensive list of patients' medications and allergies was asked as two separate questions in 2010 (one about medications and the other about allergies), but the questions were collapsed in 2011 and in subsequent years (7).
Intent to apply for Medicare or Medicaid EHR Incentive Programs: Obtained from "yes, we already applied" and "yes, we intend to apply" responses to the question: "Medicare and Medicaid offer incentives to practices that demonstrate 'meaningful use of health IT.' At this practice, are there plans to apply for these incentive payments?"
Demonstrating meaningful use: The Medicare and Medicaid EHR Incentive Programs provide incentive payments to physicians as they demonstrate meaningful use of certified EHR technology. The Centers for Medicare & Medicaid Services established the objectives for meaningful use in three stages that physicians must meet in order to receive an incentive payment. In 2014, physicians may receive incentive payments for Stage 2 if they meet 17 Core Set objectives and 3 of 6 Menu Set objectives, using certified EHR systems. The full list of Stage 2 objectives and measures is published (3). The 2013 NAMCS survey obtains information on only 14 of the 17 objectives. Trend information from 2010 is available for only 7 of the 17 objectives. The Tablepresents Stage 2 meaningful use Core Set objectives and corresponding 2013 NAMCS EHR survey items.
| Objective | 2013 NAMCS, EHR survey items on computerized capabilities |
|---|---|
| Use computerized provider order entry for medication, laboratory, and radiology orders | Ordering prescriptions and ordering lab rests |
| Generate and transmit permissible prescriptions electronically | Sending prescription orders electronically to the pharmacy |
| Record patient demographics | Recording patient history and demographic information |
| Record and chart vital signs changes | Recording and charting vital signs |
| Record smoking status | Recording patient smoking status |
| Use clinical decision support | Providing reminders for guideline-based interventions or screening tests and providing warnings of drug interactions or contraindications |
| Provide patients the ability to view online, download, and transmit their health information | Providing patients the ability to view online, download, or transmit information from their medical record |
| Provide clinical summaries for patients for each office visit | Providing patients with clinical summaries for each visit |
| Incorporate clinical lab-test results into Certified EHR Technology as structured data | EHR automatically graphing a specific patient’s lab results over time |
| Generate lists of patients by specific conditions | Generating lists of patients with particular health conditions |
| Use clinically relevant information to identify patient- specific education resources and provide those resources to the patient | Identifying educational resources for patient’s specific conditions |
| Perform medication reconciliation for patients referred to the eligible provider (EP) | Reconciling lists of patient medications to identify the most accurate list |
| Capability to submit electronic data to immunization registries or immunization information systems | Electronic reporting to immunization registries |
| Use secure electronic messaging to communicate with patients | Exchanging secure messages with patients |
| Protect electronic health information through appropriate technical capabilities | … |
| Use clinically relevant information to identify patients for preventive and follow-up care and send these patients reminders | … |
| Provide a summary care record for patients referred by EP | … |
… Category not applicable; no corresponding survey item.
NOTE: NAMCS, EHR survey is National Ambulatory Medical Care Survey, Electronic Health Records Survey.
NOTE: NAMCS, EHR survey is National Ambulatory Medical Care Survey, Electronic Health Records Survey.
Data source and methods
NAMCS, which is conducted by the Centers for Disease Control and Prevention's National Center for Health Statistics, is an annual, nationally representative survey of office-based physicians that collects information on physician and practice characteristics, including the adoption and use of EHR systems. The universe of NAMCS physicians comprises those classified as providing direct patient care in office-based practices, as well as clinicians in community health centers. Radiologists, anesthesiologists, and pathologists are excluded.
Since 2008, a supplemental mail survey on EHR systems has been conducted in addition to the core NAMCS, which is an in-person survey. In 2008 and 2009, samples of physicians in the core NAMCS and the supplemental mail survey, stratified by specialty, were chosen from selected geographic areas. Starting in 2010, the NAMCS EHR mail-survey sample size was increased fivefold to allow for state-level estimates and to produce stand-alone estimates without needing to be combined with the core NAMCS.
The 2013 estimates are from the NAMCS EHR survey with a sample of 10,302 physicians. Nonrespondents to the mail survey received follow-up telephone calls. The 2013 NAMCS EHR survey was conducted from February through June 2013. The unweighted response rate of the 2013 NAMCS EHR survey was 70% (67% weighted). A copy of the 2013 survey is available from the NCHS website.
Physicians' updated practice location information was used to generate state-level estimates. Estimates of intent to apply for incentives exclude about 1.3% of cases with missing information. Estimates of physician readiness to meet Stage 2 objectives were obtained by identifying physicians with EHRs that had all of the computerized capabilities listed in the Table.
Statements of differences in estimates are based on statistical tests with significance at the p < 0.05 level. Terms relating to differences such as "increased" or "decreased" indicate that the differences are statistically significant. Lack of comment regarding the difference does not mean that the difference was tested and found to be not significant.
About the authors
Chun-Ju Hsiao is with the Agency for Healthcare Research and Quality, and Esther Hing is with the National Center for Health Statistics.
References

Suggested citation
Hsiao C-J, Hing E. Use and characteristics of electronic health record systems among office-based physician practices:
United States, 2001–2013. NCHS data brief, no 143. Hyattsville, MD: National Center for Health Statistics. 2014.
United States, 2001–2013. NCHS data brief, no 143. Hyattsville, MD: National Center for Health Statistics. 2014.
Copyright information
All material appearing in this report is in the public domain and may be reproduced or copied without permission; citation as to source, however, is appreciated.
National Center for Health Statistics
Charles J. Rothwell, M.S., M.B.A., Director
Jennifer H. Madans, Ph.D., Associate Director for Science
Jennifer H. Madans, Ph.D., Associate Director for Science
Division of Health Care Statistics
Clarice Brown, M.S., Director




















.png)









No hay comentarios:
Publicar un comentario