
Use of Colorectal Cancer Screening Tests by State
GIS SNAPSHOT — Volume 15 — June 14, 2018
Djenaba A. Joseph, MD, MPH1; Jessica B. King, MPH1; Thomas B. Richards, MD1; Cheryll C. Thomas, MSPH1; Lisa C. Richardson, MD, MPH1 (View author affiliations)
Suggested citation for this article: Joseph DA, King JB, Richards TB, Thomas CC, Richardson LC. Use of Colorectal Cancer Screening Tests by State. Prev Chronic Dis 2018;15:170535. DOI: http://dx.doi.org/10.5888/pcd15.170535.
PEER REVIEWED
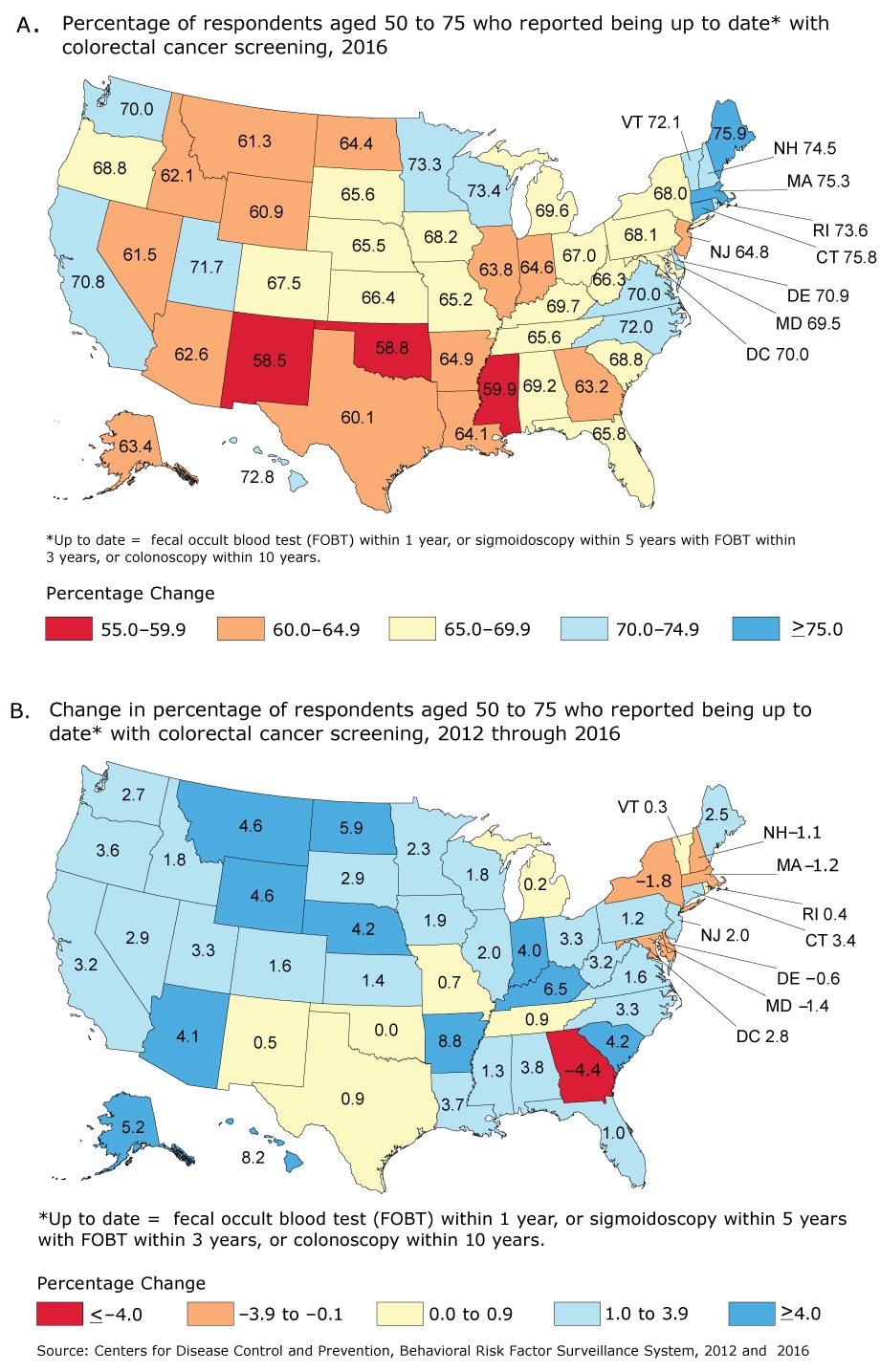
Figure. Progress toward increased use of colorectal cancer (CRC) screening tests, by state. A. Percentage of respondents aged 50 to 75 who reported being up to date with CRC screening in the 2016 Behavioral Risk Factor Surveillance System (1). The percentage up to date for the United States overall was 67.3%. B. The absolute change in percentage of respondents aged 50 to 75 who reported being up to date with CRC screening from 2012 through 2016, by state, Behavioral Risk Factor Surveillance System, 2012 (2), 2016 (1). Up to date is defined as having had a fecal occult blood test (FOBT) within the past year, sigmoidoscopy within the past 5 years with FOBT within the past 3 years, or colonoscopy within the past 10 years. Source: CDC Behavioral Risk Factor Surveillance System (BRFSS), BRFSS, 2012 and 2016 (1–2). [A tabular version of this figure is also available.]
Background
Colorectal cancer (CRC) is the second most common cause of cancer death among cancers that affect both men and women (3). There is strong evidence that screening reduces CRC incidence and deaths from the disease (4). The 2008 US Preventive Services Task Force (USPSTF) recommendations include several test options for screening for CRC among adults aged 50 to 75: 1) annual high-sensitivity fecal occult blood test (FOBT), 2) colonoscopy every 10 years, or 3) sigmoidoscopy every 5 years with FOBT every 3 years (4). Despite strong evidence for its use, an estimated 23 million age-eligible adults were not tested for CRC in 2012 (5). This article describes the estimated percentage of adults aged 50 to 75 (eligible adults) who reported being up to date with CRC screening in 2016, and the change in the percentage from 2012 through 2016, by state.
Methods
The Behavioral Risk Factor Surveillance Survey (BRFSS) is an annual, state-based, random-digit–dialed telephone survey of the civilian, noninstitutionalized adult population aged 18 or older. BRFSS collects information on health risk, behaviors, preventive-health practices, and health care access in the United States. Respondents aged 50 or older respond to questions asking if they ever had a CRC screening test and, if yes, when the most recent test was done. We analyzed data from the 2012 and 2016 BRFSS to estimate the percentage of adults aged 50 to 75 who reported having been screened for CRC screening consistent with 2008 USPSTF recommendations (up to date with CRC screening) by state (5). USPSTF recommendations were updated in 2016, but we used 2008 recommendations for our analysis. Respondents who declined to answer, had a missing answer, or who answered, “don’t know/not sure,” were excluded from the analysis. SUDAAN (RTI International) was used to account for the complex sampling design. Data were weighted to the age, sex, and racial/ethnic distribution of each state’s adult population by using intercensal estimates that were age-standardized to the 2016 BRFSS population. ArcGIS Desktop, version 10.5 (ESRI) was used to create a map series to show the percentage up to date in 2016 (Map A) and the absolute change in the percentage up to date between 2012 and 2016 (Map B).
Main Findings
The percentage of adults aged 50 to 75 who reported being up to date with CRC screening in the United States increased from 65.5% in 2012 to 67.3% in 2016. The percentage of eligible adults who were up to date with CRC screening by state ranged from 58.5% (New Mexico) to 75.9% (Maine) in 2016 (Map A).
From 2012 through 2016, 37 states had an estimated increase of 1% or more in the percentage of eligible adults who were up to date with CRC screening (Map B), with the largest in Arkansas (8.8%), followed by Hawaii (8.2%), and 10 states ranging from 4% to 6.5%. Six states had an overall estimated decrease in the percentage that were up to date with the largest decline in Georgia (−4.4%). Of the 10 states with at least 70% of eligible adults up to date in 2012, 4 had an estimated increase of 1% or more, and 4 had an overall estimated decline by 2016. Of the 15 states with 65% to 69.9% of eligible adults up to date in 2012, 12 had an estimated increase of 1% or more, and 2 had an overall estimated decline. Of the 15 states with 60% to 64.9% of eligible adults up to date in 2012, 13 had an estimated increase of 1% or more, and 4 had an estimated increase of 4% or more. Finally, of 11 states with less than 60% of eligible adults up to date in 2012, 8 had an estimated increase of 1% or more, and 6 had an estimated increase of 4% or more.
Action
Most states had an estimated increase in the percentage of eligible adults who were up to date with CRC screening from 2012 to 2016 for an overall estimated increase in CRC screening prevalence of 1.8%; this represents an estimated additional 5,095,254 people who were screened. The largest estimated gains were in states with lower (<65%) percentages of eligible adults who were up to date in 2012, whereas smaller estimated increases or declines occurred in states with higher (≥70%) percentages of eligible adults who were up to date. This suggests that as the percentage of people up to date with CRC screening increases in states, the remaining unscreened, eligible adults may be harder to reach. Previous research described several barriers to CRC screening, including lack of health insurance or a regular health care provider, failure of the provider to recommend screening, the patient’s lack of awareness or knowledge of the need to be screened, low household income, low educational attainment, and being of a racial/ethnic minority (6). Public health can play a critical role in linking hard-to-reach populations to health care systems. CDC’s Colorectal Cancer Control Program (https://www.cdc.gov/cancer/crccp/) funds 23 states, 6 universities, and a tribe to partner with primary care clinics that serve hard-to-reach populations to support the implementation of evidence-based interventions recommended by the Community Guide (https://www.thecommunityguide.org/topic/cancer) that have been shown to increase CRC screening. These programs leverage public health expertise in population health management by working with clinics to embed sustainable cancer screening processes.
Our study has 4 limitations. First, CRC screening prevalence might be overestimated or underestimated, because BRFSS does not specify whether testing was done for screening or diagnosis. Second, data were self-reported and may be subject to recall and social desirability bias. Third, our analysis did not account for sampling error, and described changes may be due to sampling error alone. Fourth, response rates were low (45.2% in 2012 and 47.1% in 2016), and respondents who did not answer all questions were excluded (6.8% in 2012, 8.9% in 2016), although BRFSS weighting procedure attempts to correct for nonresponse.
Fourteen states in the United States have reached the Healthy People 2020 objective for being up to date with CRC screening (70.5%), and most remaining states have made progress toward reaching this goal. Continued support for state and local efforts to increase CRC screening, such CDC’s Comprehensive Cancer Control Coalitions, is needed. Efforts to integrate these interventions into other preventive care and disease management practices may improve their reach and sustainability.
Acknowledgments
The findings and conclusions in this report are those of the authors and do not necessarily represent the official position of the Centers for Disease Control and Prevention.
Author Information
Corresponding Author: Djenaba A. Joseph, MD, MPH, Centers for Disease Control and Prevention, Division of Cancer Control and Prevention, 4770 Buford Hwy, MS F76, Atlanta, GA 30341. Telephone: 770-488-3157. Email: dajoseph@cdc.gov.
Author Affiliations: 1Division of Cancer Prevention and Control, Centers for Disease Control and Prevention, Atlanta, Georgia.
References
- Centers for Disease Control and Prevention. Behavioral Risk Factor Surveillance System. Atlanta, Georgia: US Department of Health and Human Services, Centers for Disease Control and Prevention, 2016. https://www.cdc.gov/brfss/annual_data/annual_2016.html. Accessed September 1, 2017.
- Centers for Disease Control and Prevention (CDC). Behavioral Risk Factor Surveillance System Survey Data. Atlanta, Georgia: US Department of Health and Human Services, Centers for Disease Control and Prevention, 2012. https://www.cdc.gov/brfss/annual_data/annual_2012.html. Accessed September 1, 2017.
- Centers for Disease Control and Prevention. National Program of Cancer Registries and Surveillance, Epidemiology, and End Results SEER Stat Database: NPCR and SEER Incidence — USCS 2001–2014 Public Use Research Database, Released August 2017, based on the November 2016 submission. www.cdc.gov/cancer/npcr/public-use. Accessed September 15, 2017.
- US Preventive Services Task Force. Screening for colorectal cancer: US Preventive Services Task Force recommendation statement. Ann Intern Med 2008;149(9):627–37. CrossRefPubMed
- Centers for Disease Control and Prevention. Vital signs: colorectal cancer screening test use — United States, 2012. MMWR Morb Mortal Wkly Rep 2013;62(44):881–8. PubMed
- Holden DJ, Harris R, Porterfield DS, Jonas DE, Morgan LC, Reuland D, et al. Enhancing the use and quality of colorectal cancer screening. Evidence report/technology assessment No.190. (Prepared by the RTI International–University of North Carolina Evidence-Based Practice Center under contract no. 290-2007-10056-I.) AHRQ publication No. 10-E-002. Rockville (MD): Agency for Healthcare Research and Quality; February 2010.






















.png)








No hay comentarios:
Publicar un comentario