
Tapping Into Multiple Data “Springs” to Strengthen Policy Streams: A Guide to the Types of Data Needed to Formulate Local Retail Tobacco Control Policy
TOOLS FOR PUBLIC HEALTH PRACTICE — Volume 16 — April 4, 2019
Allison E. Myers, PhD, MPH1,2; Kathleen Knocke, MSPH3; Jennifer Leeman, DrPH, MDiv4 (View author affiliations)
Suggested citation for this article: Myers AE, Knocke K, Leeman J. Tapping Into Multiple Data “Springs” to Strengthen Policy Streams: A Guide to the Types of Data Needed to Formulate Local Retail Tobacco Control Policy. Prev Chronic Dis 2019;16:180282. DOI: http://dx.doi.org/10.5888/pcd16.180282.
PEER REVIEWED
Abstract
In 2015, the tobacco industry spent $8.24 billion to market tobacco products in convenience stores, supermarkets, pharmacies, and other retail or point-of-sale settings. Community tobacco control partnerships have numerous evidence-based policies (eg, tobacco retailer licensing and compliance, tobacco-free–school buffer zones, eliminating price discounts) to counter point-of-sale tobacco marketing. However, deciding which point-of-sale policies to implement — and when and in what order to implement them — is challenging. The objective of this article was to describe tools and other resources that local-level tobacco use prevention and control leaders can use to assemble the data they need to formulate point-of-sale tobacco policies that fit the needs of their communities, have potential for public health impact, and are feasible in the local policy environment. We were guided by Kingdon’s theory of policy change, which contends that windows of policy opportunity open when 3 streams align: a clear problem, a solution to the problem, and the political will to work for change. Community partnerships can draw on 7 data “springs” to activate Kingdon’s streams: 1) epidemiologic and surveillance data, 2) macro retail environment data, 3) micro retail environment data, 4) the current policy context, 5) local legal feasibility of policy options, 6) the potential for public health impact, and 7) political will.
Introduction
The tobacco industry spends $8.24 billion annually marketing tobacco products in convenience stores, supermarkets, pharmacies, and other retail or point-of-sale (POS) settings (1). Exposure to tobacco marketing (eg, product displays, advertisements, price discounts) increases the likelihood that youth will start using tobacco and impedes users’ attempts to quit (2–4). In communities that have a high density of tobacco retail outlets, often measured as the spatial concentration of retail outlets in a geographic area, residents are exposed to more POS tobacco marketing and have higher tobacco use rates (5,6). Retail outlet density is disproportionately high in lower-income and African American communities, and this disproportionate density likely contributes to disparities in tobacco use and tobacco-related morbidity and mortality (7,8). Retail outlets that are close to schools increase the exposure to children and adolescents, who are more susceptible to the effects of tobacco marketing than adults (4,9).
Policies to reduce retail tobacco marketing include laws, ordinances, or resolutions to regulate tobacco product sales, placement, advertisements, prices, and price promotions. They also include licensing laws and zoning regulations to reduce the number and density of retail outlets or prohibit tobacco retail outlets near schools (10–13). The potential for communities to reduce retail marketing is evidenced by recent policy wins to reduce tobacco retailer density in San Francisco and Philadelphia, restrict menthol-flavored and candy-flavored tobacco sales in Minneapolis and Oakland, and raise the age of sale to 21 years in hundreds of US localities (14). Still, little is known about how best to support community efforts to promote retail tobacco policy change (15,16). One challenge faced by community partnerships is understanding which retail tobacco control policy options to pursue, when to pursue them, and in what order they should be pursued in their geographic area of interest (eg, city, county).
Although the evidence base for POS tobacco policies is still emerging, numerous resources exist to help communities select the most promising POS policy options (13,17–20). Given the variation in the range of POS policy options and their potential impact, communities need to draw on a variety of data to select the most promising options. In this article, we built on Kingdon’s theory of policy change (21) to identify the types of data that are essential to community decision making.
In his multiple streams theory, Kingdon posited that policy change is most likely to occur when 3 policy “streams” align: 1) a local problem is documented, 2) a policy solution is available, and 3) the political will is present to work toward a solution to the problem (21). This article describes 7 data “springs” that communities can draw on to select and promote policies in ways that align with Kingdon’s 3 policy streams and create windows of opportunity for new policy enactment. The objective of this article was to 1) describe the 7 data springs, 2) recommend existing sources and data collection and analysis tools for each spring, and 3) suggest how community partnerships might apply these data to strategically select and promote policy solutions to counter retail tobacco marketing.
The 7 Data Springs
Seven data springs can contribute to community-level efforts to align with Kingdon’s 3 streams and thereby open windows of opportunity for retail tobacco marketing policy change (Figure). The first 3 springs are 1) epidemiologic/surveillance data, 2) macro retail environment data, and 3) micro retail environment data, each contributing to Kingdon’s first policy stream — documenting the local problem. The next 3 springs are 4) the current policy context, 5) the local legal feasibility of policy options, and 6) the potential for public health impact, and they relate to Kingdon’s second stream — form a policy solution. The final spring — political will — contributes to Kingdon’s final stream. Below we describe each of the data springs and recommend existing data sources and tools for collecting and analyzing information for each spring (Table).
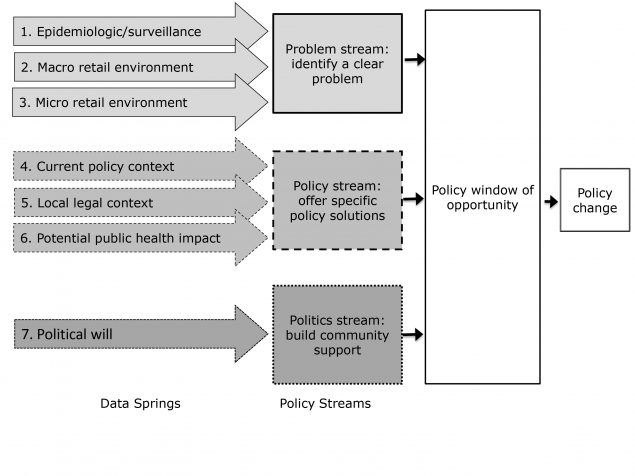
Figure.
A conceptual framework indicating data springs and policy streams that merge to create policy change. [A text version of this figure is also available.]
A conceptual framework indicating data springs and policy streams that merge to create policy change. [A text version of this figure is also available.]
Data spring 1: Epidemiologic and surveillance data
Epidemiologic and surveillance data include rates of tobacco product use and tobacco-related disability and death and the distribution of those rates across population groups in a geographic area of interest. Frequently, a geographic area of interest is a city, a county, or a group of counties. However, the focus may also be on nonincorporated areas of a county. Commonly used sources of state data include the Behavioral Risk Factor Surveillance System (BRFSS), the State Tobacco Activities Tracking and Evaluation (STATE) System, the Toll of Tobacco in the United States fact sheets available from the Campaign for Tobacco-Free Kids, and the Youth Risk Behavior Survey (YRBS). Local surveillance data are available from state health department websites; additional local tobacco indicators are available from programs such as the BRFSS’ Selected Metropolitan Area Risk Trends (SMART) project, the County Health Rankings, the 500 Cities Project, and the Big Cities Health Coalition. Key metrics are rates of tobacco product use among adults and adolescents according to such characteristics as sex; race/ethnicity; age; income; education; personal status, such as identifying as lesbian, gay, bisexual, or transgender or living with mental illness; or other characteristics that increase risk for tobacco use. Community partnerships should identify the populations who have the highest rates of tobacco use; this information can be used to educate community members and policy decision makers and to identify policy solutions with potential to eliminate disparities.
Data spring 2: Macro retail environment
Data on the macro retail environment include the number and types of tobacco retail outlets in a geographic area of interest, where they are located, and how they are clustered. Tobacco retail outlets are defined as any brick-and-mortar location that sells any type of tobacco product, including conventional combustible cigarettes and electronic devices and products with or without menthol, fruit, or other flavors. Common tobacco retail outlet types are convenience stores with or without gas stations, grocery stores, mass merchandisers, pharmacies, and tobacco-only specialty shops.
Characterization of the macro retail environment begins with obtaining or creating a list of tobacco retail outlet locations. Ideal options are to obtain a tobacco retailer licensing list or create a list by “ground truthing” or canvassing an area to identify every store that sells tobacco (22). Where licensing lists are not available, substitute lists can be derived from free or purchasable business lists from internet searches of vendors (eg, Dun and Bradstreet, Reference USA); lists of stores eligible for the policy compliance and enforcement activities of the Synar Program (www.samhsa.gov/synar) or the Food and Drug Administration; or lists of stores that sell alcohol for off-premise consumption (a proxy for a tobacco retail outlet). Tobacco tax tracking through departments of revenue may also serve as a suitable substitute list; however, only products taxed at the state level will appear on this list. Details about the sensitivity and specificity of various lists, sampling strategies, and list-cleaning protocols are published elsewhere (22,23).
The location of each retailer can then be geocoded or otherwise plotted on a map according to latitude and longitude. Beyond the number, location, and type of outlets, summary information needs to specify features or problems in the macro retail environment that are amenable to change through policy. Examples of these features include the number of retail outlets that are close (≤1,000 feet) to institutions that serve children, such as schools, parks, or child care centers, and the relationship between the number and density of tobacco retail outlets, often measured as the spatial concentration of retail outlets in a geographic area (eg, neighborhood, school zone). These analyses give a visual representation of the retail tobacco landscape and the health inequities that may be changeable with policy solutions; for example, a 1,000-feet tobacco-sales–free buffer around schools has potential to reverse disparities in density by race/ethnicity (8).
Data spring 3: Micro retail environment
A third data type includes features of the micro store environment, defined as information about the availability, price, placement, and promotion of tobacco products. Store assessments are the primary method for collecting these data and involve public health staff, community members, and other stakeholders who systematically collect observational data inside and outside retail stores. A guide to conducting store assessments is available (24). Store assessment resources are available at CounterTobacco.org, including the Standardized Tobacco Assessment for Retail Settings (STARS), with additional modules for vaping devices and electronic products (25,26). Data may include the percentage of stores in a geographic area of interest that offer tobacco price promotions (eg, cents off or multipack offers that undermine tobacco excise tax policies and promote consumption). Store assessments can be used to identify localized tobacco industry targeting (eg, lower than average prices on smokeless tobacco products in rural and low-income areas, or higher prevalence of sales of individually packaged candy-flavored or fruit-flavored tobacco products in neighborhoods with a high proportion of children). For example, in a study conducted in Milwaukee, Wisconsin, the STARS tool showed harmful POS disparities in zip codes where the population was predominantly African American and Hispanic as well as high levels of outdoor pricing and price promotion for menthol products (27). Matching localized industry targeting to policy provisions according to the STARS Policy Crosswalk (28) is an important element of formulating policy strategy.
Data spring 4: Current tobacco control policy context
This fourth data type involves cataloging state policies and characteristics to assess readiness to enact local tobacco retail marketing policies. The State of Tobacco Control state grades (American Lung Association), the State Tobacco Activities Tracking and Evaluation System (STATE), and the State Legislated Actions on Tobacco Issues (SLATI) database each offer state snapshots of tobacco control progress on established Best Practice strategies from the Centers for Disease Control and Prevention (CDC) (29). When users retrieve these data, they should first note the presence and amounts of state tax on combustible and noncombustible tobacco products and the date of the last tax increase (30). Next, users should note the strength of smoke-free rules and policies by identifying the percentage of households and people who are protected by smoke-free rules. Third, users should clarify the level of tobacco control program funding: what percentage of CDC-recommended funds are being allocated to comprehensive tobacco control programming? These data help to gauge a state’s or a locality’s readiness to work on enacting POS tobacco policies: readiness may be greatest when a state has in place robust tobacco taxes, strong smoke-free rules, and secure program funding (31). In states with lower levels of readiness, tobacco control partnerships may need to focus on raising awareness of the tobacco retail marketing problem as one component of an overall strategy to prioritize the need for continued work in tobacco control more broadly. In other words, they may need to collect data on the problem to demonstrate to decision makers exactly where and how “tobacco is not finished.” In many states, participatory community-level documentation of the retail marketing problem will serve as an energizer to the broader tobacco control movement.
Data spring 5: Local legal feasibility of policy options
A fifth data type involves understanding which retail policy solutions are feasible for the geographic area of interest, information that can be acquired through consultation with a legal technical assistance provider who specializes in tobacco control policy. A public health attorney can provide legal technical assistance and can clarify whether express or implied preemption is a barrier to progress, meaning whether existing state law precludes localities from passing certain types of tobacco control policies. A public health attorney can clarify details of existing tobacco retailer licensing policies and the extent to which they are being enforced, how they might serve as a foundation for future efforts, and the relative potential for legal success related to various policy solutions in the geographic area of interest. Public health attorneys can provide assistance in navigating policy interventions that may conflict with the First Amendment by restricting free speech through advertising or commercial speech. Contact information for legal technical assistance providers is available (Table).
Data spring 6: Potential for public health impact
Data types essential to formulating solutions are research findings on the potential of policies to reduce exposure to tobacco marketing and/or reduce the prevalence of tobacco use at the population level. In formulating a policy solution, the potential for public health impact needs to be assessed along with data from the other streams. Data from streams 1, 2, and 3 can be applied to compare each policy option’s potential for impact given the local problem. For example, the impact of retailer licensing policies to reduce the number and density of outlets will be greatest in areas that have problems with high retailer density in low-income neighborhoods or many retailers in close proximity to schools. Data from spring 5 may influence a community partnership’s decision to select a policy option that may have less evidence in support of its effectiveness than other options but has strong legal feasibility and therefore may provide an early win that the partnership can build on to create the political will needed for future efforts to enact policy solutions with potentially greater impact.
Data on policy effectiveness is emerging. Raising the price of tobacco products is the most effective way to reduce overall consumption; this principle applies to both gold-standard tax-based approaches (eg, an excise tax) and newer nontax approaches that restrict tobacco industry strategies to minimize price (32) such as prohibiting price discounts, enacting minimum price laws, or prohibiting coupon redemption (33,34). Strategies that limit the number, type, location, and density of outlets also have good evidence in support of their effectiveness at reducing exposure to tobacco marketing and smoking rates (8,35). Policies that restrict or remove tobacco product displays in retail outlets (eg, display bans) have resulted in reductions among consumers in noticing or recalling displays (36,37) and making impulse purchases (37) but no short-term change in tobacco use prevalence among adults or adolescents (36), although mathematical models suggest that these policies would reduce tobacco use over time (38). Multiple online resources provide lists of policy options together with summaries of and citations to evidence in support of their impact (Table).
Data spring 7: Amount of political will
Data on political will include data on attitudes, beliefs, and vested interest among community members and key political decision makers in POS marketing relative to other priorities (eg, maintaining a business-friendly climate) and toward POS marketing policy solutions. Information on public support for policies can be gathered through public opinion polls or focus groups and interviews (38,39). Resources for conducting public opinion surveys, such as those provided by CounterTobacco.org, guide communities through the process and help leverage results to persuade policy makers (http://countertobacco.org/resources-tools/public-opinion-surveys).
Community members’ political will is central to getting an issue on the agenda of decision-making bodies such as town councils. Community members must also have the will and ability to anticipate and prepare for industry interference in policy activities (Table). The political will of decision makers (eg, town council members, mayors) also is important. Key decision makers need to view retail tobacco policy as a pressing issue so that they will propose policy changes and support their enactment. One-on-one meetings are one strategy for understanding local decision makers’ views of tobacco retail marketing policies in general and their positions on specific strategies.
Toward Policy Change: Merging Data Springs to Activate Policy Streams
We outlined how community partnerships can draw on the 7 data springs to activate the 3 streams central to Kingdon’s theory of successful policy change. Springs 1, 2, and 3 can be tapped into to identify the local problem (Kingdon’s first stream). Engaging community members in collecting and sharing these data are a powerful tool for building political will to work for change (Kingdon’s third stream). Springs 1, 2, and 3 also contribute to policy formulation (Kingdon’s second stream) by providing local data on the problem, data that are key to selecting and targeting policy strategies to align with local needs. Springs 4 through 7 further contribute to Kingdon’s second stream by providing the data needed to stage policy strategies to fit local readiness for policy change. Spring 7 also provides data suggested to design a policy campaign to generate the political and community will needed to enact new policy (Kingdon’s third stream).
We identified 7 “springs of evidence” that are essential to local public health officials’ work to formulate the POS tobacco policies with the greatest potential to decrease the burden of tobacco use in their communities. We acknowledge that some data springs do not exist or are shallow (eg, many states do not require tobacco retailer licensing, and policy contexts are difficult to track systematically), and we encourage continued investment in data collection and sharing. To the extent possible, we also encourage policy effectiveness studies to further inform policy development.
Our model focuses on tobacco retail policy, but the conceptual data springs are applicable to other health-supporting policy initiatives. Although the sources of data may differ, and new springs may need to be added, the conceptual process of evidence-informed decision making can be applied to a range of retail policies (food, alcohol, physical activity environment). Harnessing relevant data to change local policy is key to creating health-supporting community environments and improving population health.
Acknowledgments
Funds internal to Counter Tools were used to support Dr Myers. Ms Knocke and Dr Leeman were supported by CDC and the National Cancer Institute, National Institutes of Health (NIH) through cooperative agreement no. U48 DP005017-SIP to the Center for Health Promotion and Disease Prevention at the University of North Carolina (UNC), Chapel Hill. The content is solely the responsibility of the authors and does not necessarily represent the official views of UNC, CDC, or NIH. The authors thank Pat McKone and Maggie Mahoney for comments on early manuscript drafts. Dr Myers is co-inventor of the UNC-owned Store Mapper and Store Audit Center tools and receives royalties from their distribution. Ms Knocke and Dr Leeman have no conflicts of interest to declare. This research did not involve human participants. No copyrighted materials, surveys, instruments, or tools were used to prepare this manuscript.
Author Information
Corresponding Author: Kathleen Knocke, MSPH, 1101 McGavran-Greenberg, Campus Box 7411, Chapel Hill, NC 27599. Telephone: 919-966-7350. Email: Kathleenknocke@unc.edu.
Author Affiliations: 1Counter Tools, Inc, Carrboro, North Carolina. 2Department of Health Behavior, Gillings School of Global Public Health, University of North Carolina, Chapel Hill, North Carolina. 3Department of Health Policy and Management, Gillings School of Global Public Health, University of North Carolina, Chapel Hill, North Carolina. 4School of Nursing, University of North Carolina, Chapel Hill, North Carolina.
References
- Federal Trade Commission. Federal Trade Commission cigarette report for 2011; 2013. https://www.ftc.gov/reports/federal-trade-commission-cigarette-report-2016-federal-trade-commission-smokeless-tobacco. Accessed February 6, 2019.
- Robertson L, McGee R, Marsh L, Hoek J. A systematic review on the impact of point-of-sale tobacco promotion on smoking. Nicotine Tob Res 2015;17(1):2–17. CrossRef PubMed
- Paynter J, Edwards R. The impact of tobacco promotion at the point of sale: a systematic review. Nicotine Tob Res 2009;11(1):25–35. CrossRef PubMed
- Robertson L, Cameron C, McGee R, Marsh L, Hoek J. Point-of-sale tobacco promotion and youth smoking: a meta-analysis. Tob Control 2016;25(e2):e83–9. CrossRef PubMed
- Pulakka A, Halonen JI, Kawachi I, Pentti J, Stenholm S, Jokela M, et al. Association between distance from home to tobacco outlet and smoking cessation and relapse. JAMA Intern Med 2016;176(10):1512–9. CrossRef PubMed
- Reitzel LR, Cromley EK, Li Y, Cao Y, Dela Mater R, Mazas CA, et al. The effect of tobacco outlet density and proximity on smoking cessation. Am J Public Health 2011;101(2):315–20.CrossRef PubMed
- Lee JG, Henriksen L, Rose SW, Moreland-Russell S, Ribisl KM. A systematic review of neighborhood disparities in point-of-sale tobacco marketing. Am J Public Health 2015;105(9):e8–18.CrossRef PubMed
- Ribisl KM, Luke DA, Bohannon DL, Sorg AA, Moreland-Russell S. Reducing disparities in tobacco retailer density by banning tobacco product sales near schools. Nicotine Tob Res 2017;19(2):239–44. CrossRef PubMed
- Henriksen L, Schleicher NC, Feighery EC, Fortmann SP. A longitudinal study of exposure to retail cigarette advertising and smoking initiation. Pediatrics 2010;126(2):232–8. CrossRefPubMed
- Ackerman A, Etow A, Bartel S, Ribisl KM. Reducing the density and number of tobacco retailers: policy solutions and legal issues. Nicotine Tob Res 2017;19(2):133–40. CrossRef PubMed
- National Center for Chronic Disease Prevention and Health Promotion, Office on Smoking and Health. Preventing tobacco use among youth and young adults: a report of the Surgeon General. Atlanta (GA): Centers for Disease Control and Prevention; 2012.
- Wallace RB, Stratton K, Bonnie RJ, editors. Ending the tobacco problem: a blueprint for the nation. Washington (DC): National Academies Press; 2007.
- Center for Public Health Systems Science. Point-of-sale strategies: a tobacco control guide. St Louis (MO): St Louis Center for Public Health Systems Science, George Warren Brown School of Social Work at Washington University in St Louis and the Tobacco Control Legal Consortium; 2014. https://www.publichealthlawcenter.org/sites/default/files/resources/tclc-guide-pos-policy-WashU-2014.pdf. Accessed February 6, 2019.
- Myers AE, Southwell BG, Ribisl KM, Moreland-Russell S, Lytle LA. Setting the agenda for a healthy retail environment: content analysis of US newspaper coverage of tobacco control policies affecting the point of sale, 2007–2014. Tob Control 2017;26(4):406–14. CrossRef PubMed
- Leeman J, Myers A, Grant JC, Wangen M, Queen TL. Implementation strategies to promote community-engaged efforts to counter tobacco marketing at the point of sale. Transl Behav Med 2017;7(3):405–14. CrossRef PubMed
- Leeman J, Myers AE, Ribisl KM, Ammerman AS. Disseminating policy and environmental change interventions: insights from obesity prevention and tobacco control. Int J Behav Med 2015;22(3):301–11. CrossRef PubMed
- Center for Public Health Systems Science. Policy strategies: a tobacco control guide. St Louis (MO): St Louis Center for Center for Public Health Systems Science, George Warren Brown School of Social Work at Washington University in St Louis and the Tobacco Control Legal Consortium; 2014. https://www.publichealthlawcenter.org/sites/default/files/resources/tclc-guide-tobacco-policy-strategies-WashU-2014.pdf. Accessed February 6, 2019.
- Center for Public Health Systems Science. Pricing policy: a tobacco control guide. St Louis (MO): St Louis Center for Center for Public Health Systems Science, George Warren Brown School of Social Work at Washington University in St Louis and the Tobacco Control Legal Consortium; 2014. https://www.publichealthlawcenter.org/sites/default/files/resources/tclc-guide-pricing-policy-WashU-2014.pdf. Accessed February 6, 2019.
- Tobacco Control Network. 2016 Policy recommendations guide. http://tobaccocontrolnetwork.org/tcn-policy/#policy. Accessed February 6, 2019.
- ChangeLab Solutions. Point of sale playbook. Oakland (CA): ChangeLab Solutions; 2016. http://www.changelabsolutions.org/sites/default/files/Point_of_Sale_Playbook_FINAL_20160105.pdf. Accessed February 6, 2019.
- Kingdon JW. Agendas, alternatives, and public policies. Boston (MA): Longman; 2011.
- D’Angelo H, Fleischhacker S, Rose SW, Ribisl KM. Field validation of secondary data sources for enumerating retail tobacco outlets in a state without tobacco outlet licensing. Health Place 2014;28:38–44. CrossRef PubMed
- Lee JG, Shook-Sa BE, Bowling JM, Ribisl KM. Comparison of sampling strategies for tobacco retailer inspections to maximize coverage in vulnerable areas and minimize cost. Nicotine Tob Res 2018;20(11):1353–8. CrossRef PubMed
- Feld AL, Johnson TO, Byerly KW, Ribisl KM. How to conduct store observations of tobacco marketing and products. Prev Chronic Dis 2016;13:E25. CrossRef PubMed
- State and Community Tobacco Control Research. STARS (Standardized Tobacco Assessment for Retail Settings); 2014. http://countertobacco.org/resources-tools/store-assessment-tools/. Accessed March 1, 2018.
- Henriksen L, Ribisl KM, Rogers T, Moreland-Russell S, Barker DM, Sarris Esquivel N, et al. Standardized Tobacco Assessment for Retail Settings (STARS): dissemination and implementation research. Tob Control 2016;25(Suppl 1):i67–74. CrossRef PubMed
- Laestadius L, Sebero H, Myers A, Mendez E, Auer P. Identifying disparities and policy needs with the STARS surveillance tool. Tob Regul Sci 2018;4(4):12–21. CrossRef
- Center for Public Health Systems Science. STARS policy crosswalk. https://cphss.wustl.edu/items/stars-policy-crosswalk/. Accessed March 1, 2018.
- Centers for Disease Control and Prevention. Best practices for comprehensive tobacco control programs — 2014. Atlanta (GA): US Department of Health and Human Services, Centers for Disease Control and Prevention, National Center for Chronic Disease Prevention and Health Promotion, Office on Smoking and Health; 2014.
- Chaloupka FJ, Straif K, Leon ME, Working Group, International Agency for Research on Cancer. Effectiveness of tax and price policies in tobacco control. Tob Control 2011;20(3):235–8.CrossRef PubMed
- Luke DA, Sorg AA, Combs T, Robichaux CB, Moreland-Russell S, Ribisl KM, et al. Tobacco retail policy landscape: a longitudinal survey of US states. Tob Control 2016;25(Suppl 1):i44–51.CrossRef PubMed
- Caraballo RS, Wang X, Xu X. Can you refuse these discounts? An evaluation of the use and price discount impact of price-related promotions among US adult smokers by cigarette manufacturers. BMJ Open 2014;4(6):e004685. CrossRef PubMed
- Golden SD, Farrelly MC, Luke DA, Ribisl KM. Comparing projected impacts of cigarette floor price and excise tax policies on socioeconomic disparities in smoking. Tob Control 2016;25(Suppl 1):i60–6. CrossRef PubMed
- Golden SD, Smith MH, Feighery EC, Roeseler A, Rogers T, Ribisl KM. Beyond excise taxes: a systematic review of literature on non-tax approaches to raising tobacco product prices. Tob Control 2015;25(4):377–85. CrossRef PubMed
- Myers AE, Hall MG, Isgett LF, Ribisl KM. A comparison of three policy approaches for tobacco retailer reduction. Prev Med 2015;74:67–73. CrossRef PubMed
- McNeill A, Lewis S, Quinn C, Mulcahy M, Clancy L, Hastings G, et al. Evaluation of the removal of point-of-sale tobacco displays in Ireland. Tob Control 2011;20(2):137–43. CrossRefPubMed
- Li L, Borland R, Fong GT, Thrasher JF, Hammond D, Cummings KM. Impact of point-of-sale tobacco display bans: findings from the International Tobacco Control Four Country Survey. Health Educ Res 2013;28(5):898–910. CrossRef PubMed
- Farley SM, Coady MH, Mandel-Ricci J, Waddell EN, Chan C, Kilgore EA, et al. Public opinions on tax and retail-based tobacco control strategies. Tob Control 2015;24(e1):e10–3. CrossRefPubMed
- Rose SW, Emery SL, Ennett S, McNaughton Reyes HL, Scott JC, Ribisl KM. Public support for family smoking prevention and tobacco control act point-of-sale provisions: results of a national study. Am J Public Health 2015;105(10):e60–7. CrossRef PubMed






















.png)








No hay comentarios:
Publicar un comentario