NCHS Data Brief
Number 101, August 2012
The Health of Male Veterans and Nonveterans Aged 25–64: United States, 2007–2010
On This Page
- Key findings
- On a general health measure, veterans were more likely than nonveterans to report fair or poor health.
- Veterans were more likely than nonveterans to report experiencing two or more out of nine chronic conditions.
- Veterans reported serious psychological distress more often than nonveterans.
- Veterans reported work limitations more often than nonveterans.
- Veterans were more likely than nonveterans to have health insurance.
- Summary
- Definitions
- Data source and methods
- About the authors
- References
- Suggested citation
 (616 KB)
(616 KB)Ellen A. Kramarow, Ph.D., and Patricia N. Pastor, Ph.D.
Key findings
Data from the National Health Interview Survey, 2007–2010- Veterans were more likely than nonveterans to report having two or more chronic conditions.
- Veterans reported serious psychological distress more often than nonveterans; but less than 5% of both veterans and nonveterans reported serious psychological distress.
- Veterans had work limitations more often than nonveterans.
- Veterans were more likely than nonveterans to have health insurance.
More attention is now being paid to gathering accurate data to help veterans readjust to civilian life (3). Many studies of veterans only use information from military or veteran databases, which limits the ability to make comparisons with the overall population. This report uses data from the 2007–2010 National Health Interview Survey (NHIS) to describe the health status of community-dwelling male veterans aged 25–64. It directly compares the health status of veterans with nonveterans on a variety of measures.
Keywords: chronic conditions, serious psychological distress, health insurance
On a general health measure, veterans were more likely than nonveterans to report fair or poor health.
- The percentage of veterans and nonveterans reporting fair or poor health was similar among men aged 25–44 and men aged 55–64 (Figure 1).
- Among men aged 25–64, 16% of veterans reported being in fair or poor health, compared with 10% of nonveterans. Among men aged 45–54, a higher percentage of veterans reported being in fair or poor health (17% compared with 12%).
- Reporting fair or poor health increased with age for both veterans and nonveterans.
Figure 1. Fair or poor health status among men aged 25–64, by age group and veteran status: United States, 2007–2010
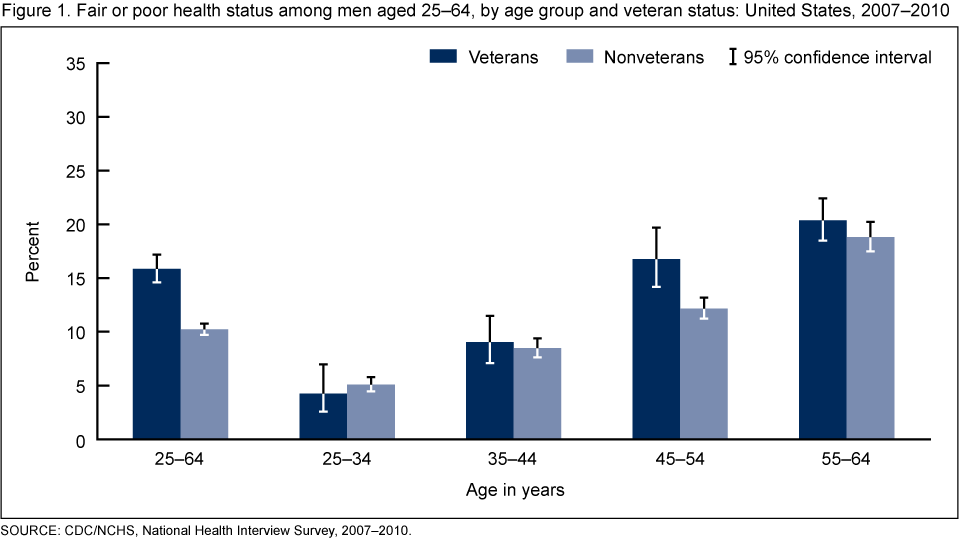
SOURCE: CDC/NCHS, National Health Interview Survey, 2007–2010.
Veterans were more likely than nonveterans to report experiencing two or more out of nine chronic conditions.
- The prevalence of two or more chronic conditions was lowest for men aged 25–34 (3%) and increased with age (Figure 2).
- Veterans aged 45–64 were significantly more likely than nonveterans to report experiencing two or more chronic conditions (19% compared with 13% for ages 45–54, and 31% compared with 25% for ages 55–64).
Figure 2. Two or more chronic conditions among men aged 25–64, by age group and veteran status: United States, 2007–2010
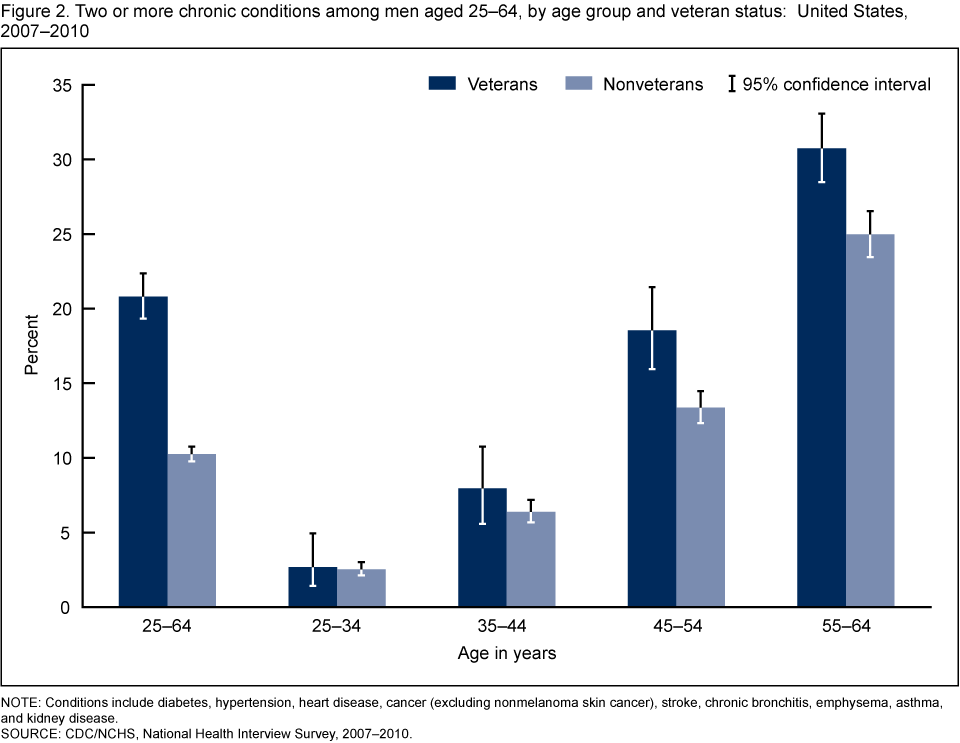
NOTE: Conditions include diabetes, hypertension, heart disease, cancer (excluding nonmelanoma skin cancer), stroke, chronic bronchitis, emphysema, asthma, and kidney disease.
SOURCE: CDC/NCHS, National Health Interview Survey, 2007–2010.
SOURCE: CDC/NCHS, National Health Interview Survey, 2007–2010.
Veterans reported serious psychological distress more often than nonveterans.
- Overall, less than 5% of veterans and nonveterans aged 25–64 reported serious psychological distress, but the percentage among veterans was higher than among nonveterans (Figure 3).
- Veterans aged 45–54 reported a higher percentage of serious psychological distress than nonveterans (5% compared with 3%).
- Among men aged 25–44 and 55–64, the percentage of veterans and nonveterans reporting serious psychological distress was not significantly different.
Figure 3. Serious psychological distress among men aged 25–64, by age group and veteran status: United States, 2007–2010
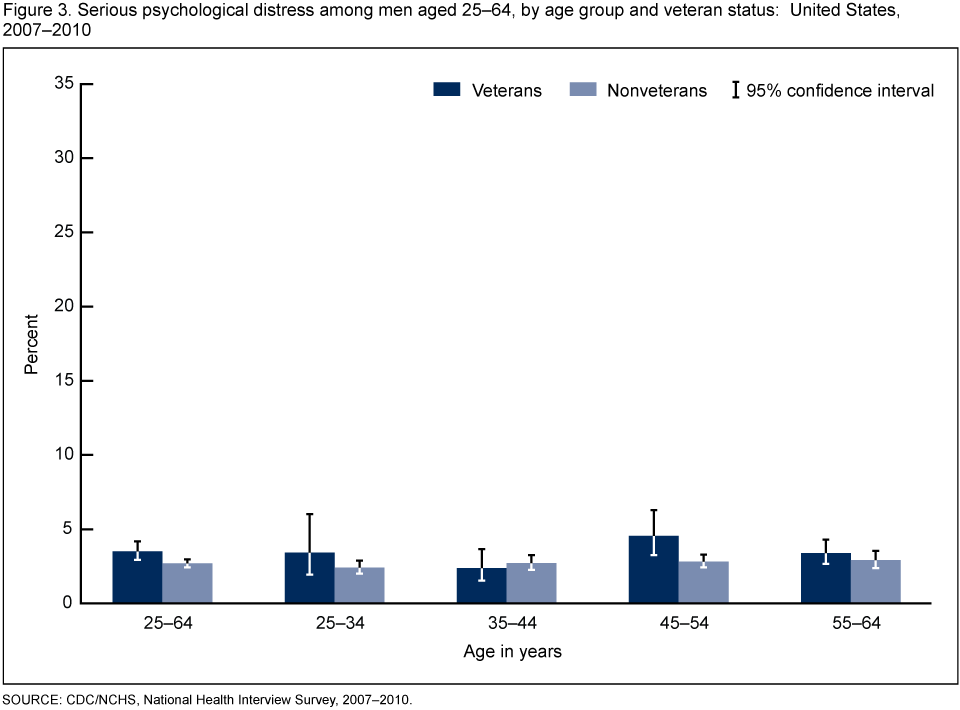
SOURCE: CDC/NCHS, National Health Interview Survey, 2007–2010.
Veterans reported work limitations more often than nonveterans.
- Overall, veterans aged 25–64 were more likely than nonveterans to report work limitations (18% compared with nearly 10%) (Figure 4).
- Among men aged 25–34, small and similar percentages of veterans (5%) and nonveterans (6%) reported work limitations. However, among men aged 35–64, veterans reported work limitations more often.
- The largest difference between the work limitations of veterans and nonveterans was observed among men aged 45–54 (19% compared with 11%).
Figure 4. Work limitations among men aged 25–64, by age group and veteran status: United States, 2007–2010
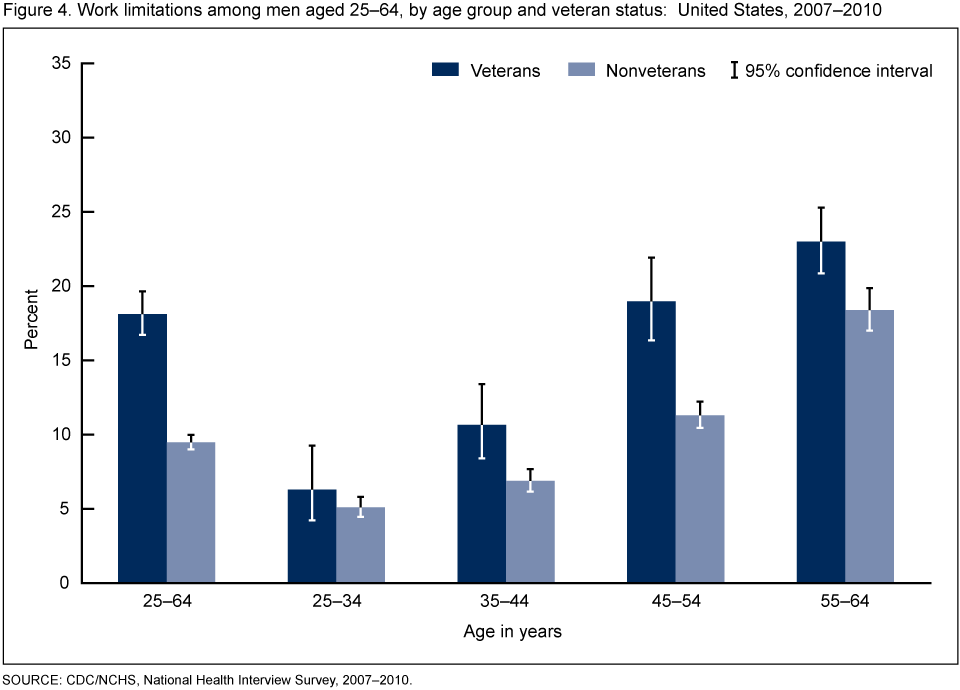
SOURCE: CDC/NCHS, National Health Interview Survey, 2007–2010.
Veterans were more likely than nonveterans to have health insurance.
- Nearly 90% of veterans aged 25–64 had health insurance (Figure 5).
- Among all age groups, veterans were more likely than nonveterans to have health insurance.
- Health insurance coverage increased with age for both veterans and nonveterans.
Figure 5. Health insurance coverage among men aged 25–64, by age group and veteran status: United States, 2007–2010
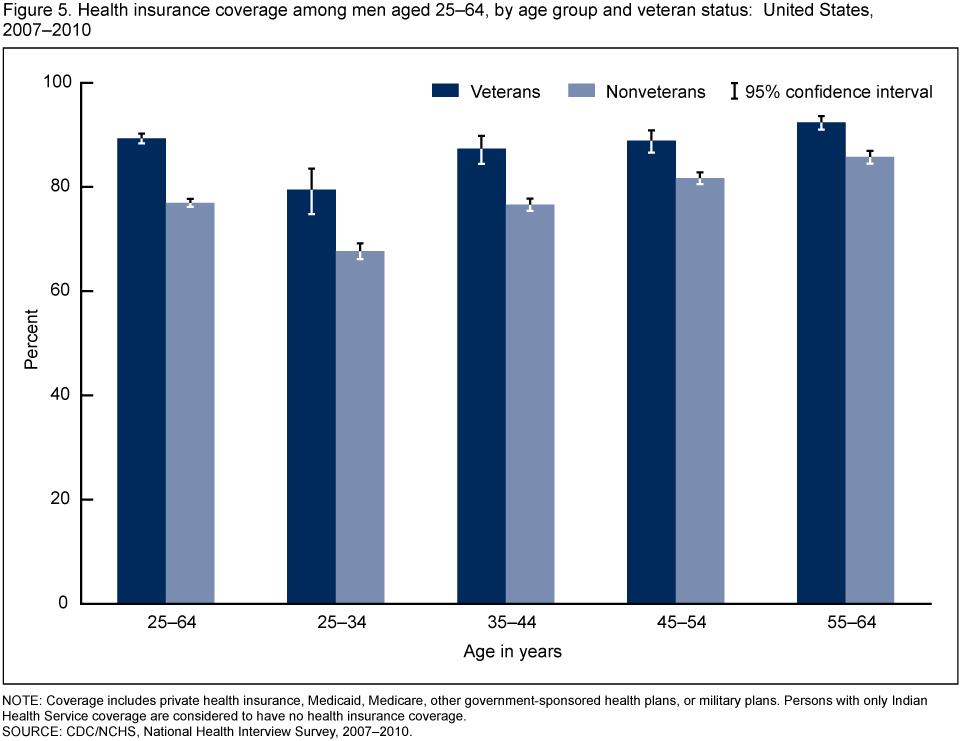
NOTE: Coverage includes private health insurance, Medicaid, Medicare, other government-sponsored health plans, or military plans. Persons with only Indian Health Service coverage are considered to have no health insurance coverage.
SOURCE: CDC/NCHS, National Health Interview Survey, 2007–2010.
SOURCE: CDC/NCHS, National Health Interview Survey, 2007–2010.
Summary
A snapshot view of the health of nonelderly veterans reveals a mixed picture of their health and functioning. Overall, veterans aged 25–64 appear to be in poorer health than nonveterans, although not all differences in health are significant for all age groups. When age differences are examined, only veterans aged 45–54 are significantly more likely than nonveterans to report fair or poor health and serious psychological distress. Other health disadvantages for veterans (e.g., the prevalence of two or more chronic conditions) appear at age 45 and over. Differences in work limitations between veterans and nonveterans are seen beginning at age 35. However, the measures presented here do not reveal major health differences between male veterans and nonveterans aged 25–34.The health differences that appear at older ages suggest that the effects of military service on health may appear later in life. Veterans also differ from nonveterans in some sociodemographic characteristics, and these characteristics may be related to observed differences in their health and functioning. Veterans are more likely to have health insurance, which may influence their access to health care and the likelihood of being diagnosed with various conditions.
The health measures presented here are not inclusive of all possible differences in health and functioning. Specifically, the measure of mental health in this report, although associated with anxiety disorders and depression, identifies only people with the most severe psychological distress (4–6). Other measures of mental health that capture a wider range of mental disorders might show more differences between veterans and nonveterans.
The sampling universe of NHIS does not include homeless people or the institutionalized population (e.g., people in long-term care facilities or in prison), which excludes some severely ill people (veterans and nonveterans) from our analysis. Addressing the problem of homelessness among veterans is a priority of the Veterans Administration (7).
This analysis is also limited in that it excludes certain other groups. The suffering of younger veterans returning from overseas with significant injuries and stress-related disorders is the focus of increased public attention. However, the number of veterans aged 18–24 included in NHIS was not large enough to support estimates for this age group. Although the percentage of women serving in the military has been steadily increasing, the relatively small numbers of female veterans also precluded their inclusion in this report.
Definitions
Veteran: Veterans are self-identified in NHIS. In the Family Core component of the survey, respondents are asked if they or any family members have "ever been honorably discharged from active duty in the U.S. Army, Navy, Air Force, Marine Corps, or Coast Guard?"Fair or poor health: Respondents are asked about their health and the health of other family members, specifically, whether their "health in general is excellent, very good, good, fair or poor?"
Serious psychological distress: The serious psychological distress scale (K6) instrument is a measure of psychological distress associated with unspecified but potentially diagnosable mental illness. Serious psychological distress during the past 30 days is defined as a score of 13 or higher on the K6 instrument (4).
Chronic condition: Respondents are asked if they had ever been told by a doctor that they had certain chronic conditions. For this report, nine conditions are considered: diabetes, hypertension, heart disease, cancer (excluding nonmelanoma skin cancer), stroke, chronic bronchitis, emphysema, asthma, and kidney disease.
Work limitation: Respondents are asked whether they or any family members are "limited in the kind or amount of work they can do because of a physical, mental, or emotional problem?"
Data source and methods
Data from the 2007–2010 NHIS were combined for this analysis. NHIS data are collected continuously throughout the year for the Centers for Disease Control and Prevention's (CDC) National Center for Health Statistics (NCHS), by interviewers from the U.S. Census Bureau. NHIS collects information about the health and health care of the civilian noninstitutionalized U.S. population. Interviews are conducted in respondents' homes, but follow-ups to complete interviews may be conducted over the telephone. The Family Core component collects information on all family members, and the Sample Adult component collects additional data on a randomly selected adult. Some information presented in this data brief was reported by a family respondent in the Family Core component of the survey. Questions on serious psychological distress and selected chronic conditions were self-reported by the sample adult. All estimates in this report are based on data for sample adults.NHIS is designed to yield a sample representative of the civilian noninstitutionalized population of the United States, and this analysis uses weights to produce national estimates. Point estimates and estimates of corresponding variances for this analysis were calculated using SUDAAN software to account for the complex sample design of NHIS. All estimates shown in this report have a relative standard error less than or equal to 30%. Differences between percentages were evaluated using two-sided significance tests at the 0.05 level with no adjustment for multiple comparisons. Terms such as "higher than" and "less than" indicate statistically significant differences. Terms such as "similar" and "no difference" indicate that the statistics being compared were not significantly different. Lack of comment regarding the difference between any two statistics does not necessarily suggest that the difference was tested and found to be not significant. For further information about NHIS and the questionnaire, visit the NHIS website.
About the authors
Ellen A. Kramarow and Patricia N. Pastor are with the CDC's National Center for Health Statistics, Office of Analysis and Epidemiology.References
- Wilmoth JM, London AS, Parker WM. Military service and men's health trajectories in later life. J Gerontol B Psychol Sci Soc Sci. 65(6):744–55. 2010.
- U.S. Department of Veterans Affairs. Veteran population 2007
.
- Institute of Medicine. Returning home from Iraq and Afghanistan: Preliminary assessment of readjustment needs of veterans, service members, and their families. Washington, DC: The National Academies Press. 2010.
- Kessler RC, Barker PR, Colpe LJ, Epstein JF, Gfroerer JC, Hiripi E, et al. Screening for serious mental illness in the general population. Arch Gen Psychiatry 60(2):184–9. 2003.
- Pratt LA. Serious psychological distress, as measured by the K6, and mortality. Ann Epidemiol 19(3):202–9. 2009.
- Reeves WC, Strine TW, Pratt LA, Thompson W, Ahluwalia I, Dhingra SS, et al. Mental illness surveillance among adults in the United States. MMWR Surveill Summ 60(Suppl 3):1–29. 2011.
- U.S. Department of Veteran Affairs. Homeless veterans
Suggested citation
Kramarow EA, Pastor PN. The health of male veterans and nonveterans aged 25–64: United States, 2007–2010. NCHS data brief, no 101. Hyattsville, MD: National Center for Health Statistics. 2012.Copyright information
All material appearing in this report is in the public domain and may be reproduced or copied without permission; citation as to source, however, is appreciated.National Center for Health Statistics
Edward J. Sondik, Ph.D., DirectorJennifer H. Madans, Ph.D., Associate Director for Science
Office of Analysis and Epidemiology
Jennifer H. Madans, Ph.D., Co-Acting DirectorJames Craver, M.A., Co-Acting Director





















.png)








No hay comentarios:
Publicar un comentario